
Date: Mon, 21 Feb 2000 11:08:54 +0500
Subject: Talus fracture
Hello all,
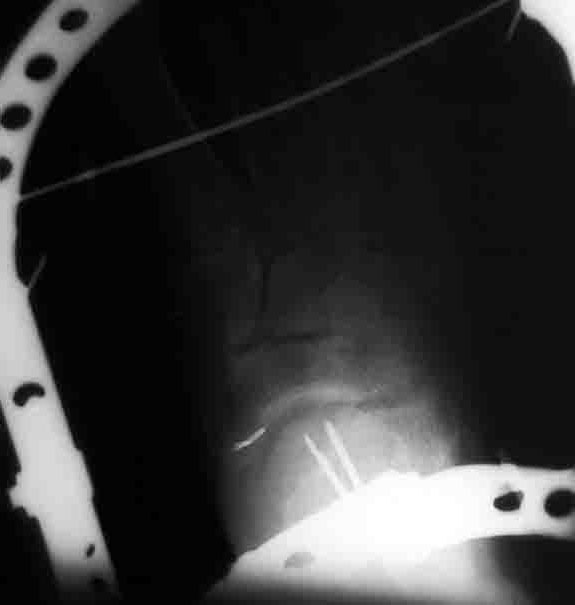
I want to submit a case. A patient after car accident (was inside) got multiple injuries. The question focused on his talar neck and facet fracture which can be seen below.
Other injuries on the leg are a) trochanteric fracture, b) multifragmentary open fracture of patella - no pus at the moment but some skin necrosis and granulations below the patella and around the tuberosity, c) midshaft fracture of tibia/fibula, d) fracture of II-IV metatarsal bones. Add also 25 days after the injury - he just transferred to us from a small town.
I presume external fixation of all injuries. What would you do with the foot?
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, str.Bankovsky, 7. Ekaterinburg 620014 Russia
|
Date: Mon, 21 Feb 2000 08:52:53 +0100
From: bruce meinhard
Dear Alex:
The foot seems to have a non-displaced fracture of the talar neck. I had only one view to examine in your email attachment.
The fracture is not displaced, but a CT scan would be very helpful to define any loose fragments or articular incongruity. This is particularly necesary if there is a rotational deformity through the fracture. A "Canale" view would also be helpful.
Most would place percutaneous cannulated antegrade or retrograde screws to hold position when the fracture is not displaced. An alternative would be casting or even extension of external fixation through the calcaneus and metatarsals to prevent motion above and below the fracture site. Open reduction, usually through two incisions, would be the procedure for a displaced injury.
BPM
Date: Mon, 21 Feb 2000 09:55:26 -0700
From: Thomas A. DeCoster M.D.
I agree image shows a minimally displaced talar neck fracture and an oblique (Canale) view would be helpful. Patient is 4 weeks post injury with ipsilateral femur, patella, tibia and metatarsal 2-4 fractures.
The comment about "presumed external fixation" confuses me as it is unclear where external fixator pins have been placed.
Regarding the foot I would consider nonoperative treatment of the minimally displaced talar neck fracture with some form of splint or cast for 8-12 weeks. If the metatarsal fractures are shaft then the same splint would treat them. If the metatarsal fractures involve the tarso-metatarsal joint (Lisfranc injury) then open treatment would be considered.
If you think there is advantage in stabilization of the talus (due to concern over loss of reduction or mobilization of the patient or mobilization of the ankle) then I would consider posterior approach with 2 x 4.0 cannulated screws (reference "Posterior approach for internal fixation of talar neck fractures Operative Techniques in Orthopedics Vol 4 No 3 1994, p 165-168)
tom decoster
Date: Mon, 21 Feb 2000 21:58:51 +0500
From: Alexander Chelnokov
Hello bruce,
Monday, February 21, 2000, 12:52:53 PM, you wrote:
bm> The foot seems to have a non displaced fracture of the talar neck.
What could you say about talo-calcaneal relations seen at the image?
bm> I had only one view to examine in your email attachment.
Yes, i attached a most informative view.
bm> The fracture is not displaced, but a CT scan would be very helpful
I decreased image size, and maybe it became less visible that there is an impressed anterior facet of the talus.
I would also be interested whether somebody suppose primary talocalcaneal fusion as an option for case like this?
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 21 Feb 2000 18:16:02 +0100
From: schandelmaier.peter
I think the talus might be subluxed in the posterior facet of the calcaneus. How about a Brodens and AP view as well as a Canale view if a CT scan is difficult.
In my opinion the Canale view in injured feet is very difficult to obtain
I think the posterior facet joint might need reduction.
peter schandelmaier, hannover
Date: Mon, 21 Feb 2000 22:45:26 +0500
From: Alexander Chelnokov
Hello Thomas,
Monday, February 21, 2000, 9:55:26 PM, you wrote:
TADMD> I agree image shows a minimally displaced talar neck fracture and an oblique (Canale) view would be helpful.
I have no copy of the image at home but i clicked the link Bill Burman kindly pointed - i again see anterior facet impression and anterior foot subluxation.
TADMD> The comment about "presumed external fixation" confuses me as it is unclear where external fixator pins have been placed.
;-) I mean external fixation for all other injuries - trochanteric and tibial shaft. Except the patella - they performed a circular suture of the extensor apparatus and bone fragments look to be close to one another, and also excessive skin necroses make to postpone any open surgery here.
TADMD> Regarding the foot I would consider nonoperative treatment of the minimally TADMD> displaced talar neck fracture with some form of splint or cast for 8-12 weeks.
If foot reduction would be easily reached and maintaned.
THX for the suggestions!
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 21 Feb 2000 21:52:55 +0100
From: Robin Peter
Dear Alex
The lateral view of this foot shows a talar neck fracture with at least 1 cm of displacement as well as a significant luxation of the posterior subtalar joint. In my opinion, if soft parts are OK, this case would require open reduction and internal fixation.
Since being within 4 weeks of the injury, we would not consider primary subtalar fusion.
We would probably use a anteromedial exposure to reduce the neck fracure and eventually a small posterolateral incision to insert a cancellous screw through the talus body into the neck for fixation.
I suspect a fracture of the lateral process of the talus to be associated in this case (this has to be confirmed on an AP view of the ankle). If confirmed, I would associate a lateral incision and ORIF of this fragment during the same procedure.
Dr Robin PETER, Clinique d'Orthopedie, Hopital Cantonal Universitaire, 1211 Geneva, Switzerland
Date: Mon, 21 Feb 2000 15:42:38 -0600
From: Gregory J Schmeling
I agree with Bruce. But, at four weeks the end may be determined. Get CT or Canale view to determine position of neck. If reasonable cast until healing, wait to walk per other fractures, if painful; fuse, if not painful you win. If sig. displacement and little callous then open, reduce, and fix.
Difficult to offer opinion based on single radiograph.
Gregory J Schmeling
Date: Mon, 21 Feb 2000 21:41:48 EST
From: edward harvey
This is a displaced fracture with some crush element to the neck region as well as a subluxation of the posterior facet. It will be difficult to reduce through anything other than simultaneous medial and lateral approaches. It will probably require plate fixation rather than lag screw fixation to maintain the facet relationships. A CT scan would be helpful in determining if you have to go through the whole exercise or do something more minimal.
Edward J Harvey MDCM FRCSC, Hand and Microvascular/Trauma, McGill University -MUHC, Montreal Qc
Date: Tue, 22 Feb 2000 10:18:52 +0100
From: bruce meinhard
I can only state that my computer may need an upgrade and my computer skills are at the rudimentary stage. Perhaps these will improve in the future.
Of course if the fracture was more displaced than I could evaluate from my image, then orif, but not primary arthrodesis, would also be my treatment of choice. If the soft tissue was not tolerant of intervention at present, then I would wait it out and when the tissue envelope was hospitable, I would do a reconstructive procedure.
BPM
Date: Tue, 22 Feb 2000 22:46:26 +0500
From: Alexander Chelnokov
Hello bruce,
Tuesday, February 22, 2000, 2:18:52 PM, you wrote:
bm> image, then orif, but not primary arthrodesis would also be my treatment of choice. If the soft tissue was not tolerant of intervention at present, then I would wait it out and when the tissue envelope was hospitable,
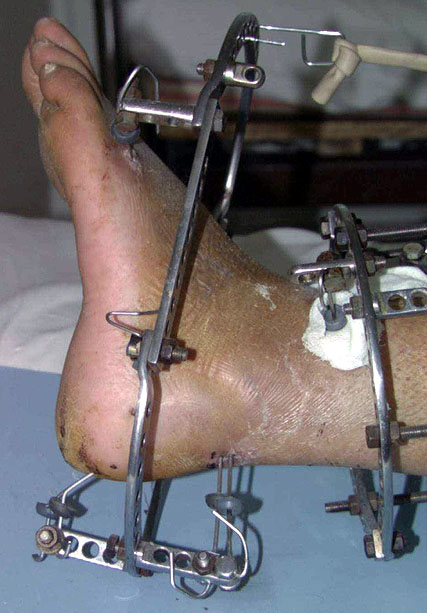
THX for the suggestions. In one procedure were performed closed reduction and ex-fix of fractures.
About the foot - its plantar flexion helped to reduce the subluxation. The neck looked also more attractive in this position. So i fixed it with two pair of wires - a couple from posterolateral side to the neck, another pair - through calcaneus and posterior facet - without the wires it would be needed to fix the foot in maximal equinus to prevent subluxation recurrence. Depressed part of the anterior facet stayed in place :-(
Tomorrow i'll prepare and send images.
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 22 Feb 2000 16:23:42 -0600
From: Giorgos Savvides
It seems that there is also a fracture of the os Calcis that brought the posterior facet forward. The body of the Talus is in the right place
Talus having been deprived of its blood supply through the neck and possibly isolated also from below, is in very high danger of ending up in avascular necrosis. Any surgical interference should not make this worse.
Suggestion: Relocate the Calcaneal facet using Ilizarov (you are the expert- I am still learning). Reduce the fracture neck of talus by putting the foot in extreme plantar flexion and retain it there by plaster, splint or EFix
G. Savvides
Date: Wed, 23 Feb 2000 09:55:39 -0700
From: Thomas A. DeCoster M.D.
On closer inspection I can see what appears to be a second fracture fragment of the talus involving the subtalar joint. It appears to be displaced 2 mm and of sufficient size to be "fixable". I don't recall ever seeing this specific pattern before and the next step would certainly be to obtain a CT scan. Perhaps this is a lateral process of the talus fracture in which case I would treat according to Hawkins (excise if small or comminuted, fix if large). If it is some other aspect of the subtalar joint I would try to reduce and fix it and bone graft the region into which it is impacted on a theoretical (displaced intra-articular fracture) basis rather than any specific evidence that this operation will improve the outcome. For me, I would definitely need a CT scan here.
TOM DECOSTER
Date: Wed, 23 Feb 2000 14:17:47 +0500
From: Alexander Chelnokov
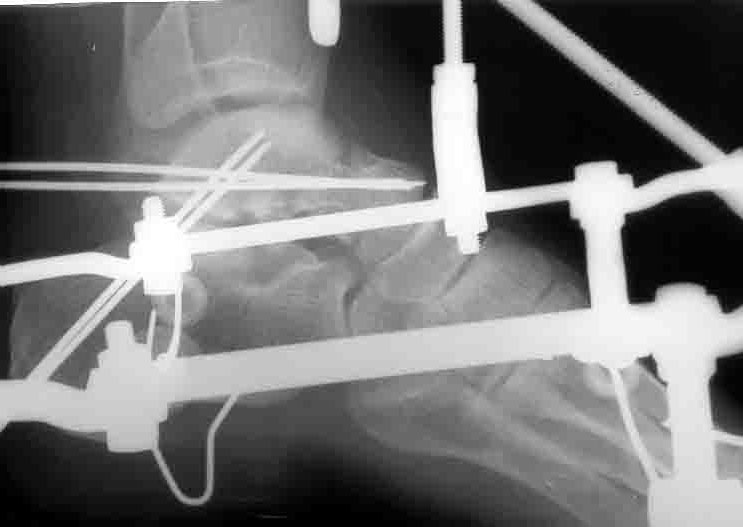
Postop Xray is attached. Sorry, axial view is of poor quality.
 |
 |
 |
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 23 Feb 2000 12:40:58 -0700
From: Thomas A. DeCoster M.D.
Nice job
I underestimated the amount of deformity of the talus initially. Where was that piece of talus/subtalar joint and how did you reduce it? Do you think the calcaneus was fractured, as someone suggested? Do you think the talus is subluxated anteriorly a bit in the ankle joint on current lateral xray?
Tom DeCoster
Date: Wed, 23 Feb 2000 06:11:31 +0100
From: bruce meinhard
Much improved reduction with no risk to the soft tissues.
BPM
Date: Thu, 24 Feb 2000 23:22:36 +0500
From: Alexander Chelnokov
Hello Thomas,
TADMD> I underestimated the amount of deformity of the talus initially. Where was that piece of talus/subtalar joint and how did you reduce it?
I didn't do anything except extreme plantar flexion. So i don't know where the piece is ;-). More precisely, it looks like some impression of the anterior facet is present, so taking in account the time since injury my opinion would be that open surgery could be more harmful than useful. So i suppose things to be as was presumed by a colleague here - if no pain here - we win, if pain after healing - go to subtalar fusion.
TADMD> Do you think the calcaneus was fractured, as someone suggested?
It seems to me no.
TADMD> Do you think the talus is subluxated anteriorly a bit in the ankle joint on current lateral xray?
Yes, sure - but it is no problem, it is just due to connection between two external fixators, i can reconfigure it in any moment.
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 9 Mar 2000 16:46
From: Bill Burman
Colleagues
I believe a problem has become apparent in the "talar neck fracture" correspondence with Alexander Chelnokov of Ekaterinburg, Russia - a participant in discussions on the OTA list with many interesting contributions for over 5 years.
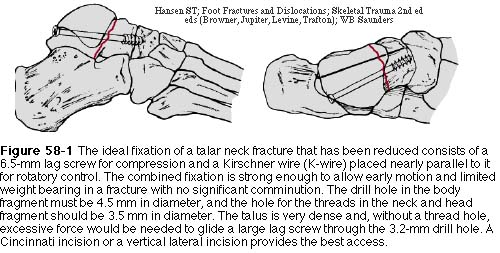
Having noted reasonable soft tissue conditions in the recent clinical photograph of the foot and the Hawkins 2 - 50% possibility of talar body avascular necrosis which would undoubtedly inhibit healing of the talar neck , I was curious to know when he would consider using a more standard screw (as depicted in Ted Hansen's chapter in "Skeletal Trauma") versus K-wire fixation.
He replied that although he has the AO Manual in Russian, there are no screws to be found in his OR.
As a way of minimally racheting up the functionality of this list, I wonder if there is someone out there who
It might break the machine if you try to send it as an attachment but I believe DHL can get it there in about a week for $20-30.
Bill Burman, MD, HWB Foundation
{kind=link}
{kind=link}
{kind=link}