
Date: Sat, 30 Jun 2001 23:45:56 +0600
Subject: Radial non-union after plating
Hello all,
A male 42 years old, an anesthesiologist, was operated in a city hospital 11 month ago - ORIF of the radial shaft. All seemed to be OK, but last three months he marked pain and mobility at the fracture site. I viewed him and found apparent clicking when pressed over the plate as well as while rotation. He has flex/ext deficiency about 10-15 degrees in both directions, and almost full range of rotation. Recent x-rays (attached) also shows slight radial shortening which wasn't present at previous films. He still can work but strongly inclined to solve the non-union. I plan to remove the plate and insert a titanium nail, maybe with grafting. What is your opinion about the case?
|
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sat, 30 Jun 2001 14:48:13 -0400
From: Kevin Pugh
Alex,
A more conventional idea for a radius non-union would be removal of the plate, debridement of the nonunion, and revision plating with bone graft. The key is to get the radius back out to length so that the distal radioulnar joint is reduced. I would recommend a plating technique that is better planned than the one you illustrate.
IM nails are effective in the hands of some surgeons for acute fractures, and with the right fracture pattern. IM nailing of the forearm is an idea that has come, and gone, and come again a few times. It certainly isn't the gold standard, and I don't think it can be recommended for a mal-nonunion.
KP
Date: Sat, 30 Jun 2001 19:37:26 -0400
From: Dr. Manuel Sotelo
Alexander The plate is too short for stability. I would use a larger plate ( 4-6 holes in each side)and graft. The nail would not give you as much stability as a plate.
Regards
Manuel Sotelo
Date: Sat, 30 Jun 2001 22:12:47 -0400
From: edward harvey
Replate the fracture. Nails have more nonunions than plates basically. There was insufficient fixation. The lag screw is not through the other cortex and the more prox screw is only through one cortex.
Literature is not ideal on what constitutes adequate CLINICAL stability but I have include one reference from CORR. He needed 9-10 cortices of fixation and has only recieved 5-6 and therefore has a nonunon. Rule-out infection and replate.
Clin Orthop 1983 May;(175):25-9 Related Articles, Books
>Complications of plate fixation of forearm fractures.
Stern PJ, Drury WJ.
Sixty-four adult patients (87 diaphyseal forearm fractures) were treated by plating. Thirty-nine percent of the fractures were classified as single bone fractures (16% radius, 23% ulna); 43% were both radial and ulnar fractures, and 19% were Galeazzi or Monteggia fracture-dislocations. A major complication occurred in 18 (28%) patients. Nonunion occurred in six patients: three of 18 bones treated with four screws (17%), but only three of 69 bones fixed with five or more screws (4.3%), a nonunion rate four times higher for bones plated with four screws. Screws loosened in three fractures, all involving the ulna. Radioulnar synostosis occurred in seven forearms, and in five of these the forearm injuries were associated with multiple system trauma involving head injury. Two patients had osteomyelitis. Both were victims of massive crush injury and delayed internal fixation, and both required removal of the implant; but eventually the fractures healed. Plate fixation of forearm fractures can have a high complication rate. Meticulous attention to surgical technique and the use of plates long enough to provide secure fixation can not be overemphasized. An increased incidence of synostosis in polytrauma, head-injured patients was noteworthy.
Edward J Harvey MDCM FRCSC
Hand and Microvascular / Trauma
Director Fracture/Bone Metabolism
Jo Miller Research Laboratories
McGill University -MUHC
Division of Orthopaedic Surgery
Montreal Qc H3G 1A4
Date: Sat, 30 Jun 2001 20:26:56 -0400
From: bruce meinhard
Alex,
replate and autogenous bone graft. Plate dorsally as a tension band. If by distraction you cannot achieve radial length as compared to the contralateral limb, shorten the ulna to restore the variance. If needed you can stage it to rule out infection and second stage after distraction, do the plating and grafting.
BPM
Date: Sun, 01 Jul 2001 22:25:27 +0200
From: Jose M. Palomo
Dear Alex,
I nail every "fresh" forearm diaphysial fracture so I really understand your will. But the only sound way I have found when treating a non-union is a well-fitted plate either with bone grafting or not.
I think, as other members of the list have pointed out, several mistakes were comitted by the first surgeon. Given you have to expose the non-union for plate removal, do no more harm to the endosteum, dont mess in a dificult nailing nearly one year after and just replate with a sound technique.
Jose M. Palomo, MD
Med. Adjunto ( Consultant Trauma & Orth. Surgeon )
Castello General Hospital
SPAIN
Date: Mon, 02 Jul 2001 09:46:28 -0500
From: Adam Starr
Alex,
I think the original ORIF wasn't so hot.
I would replate it. Open it, remove the old hardware, debride and culture the wound. Then do your best to bring it out to the right length (maybe compare to films of the contralateral side) and plate it again. I'd get 8 cortices on either side of the fracture. Then I'd bone graft it.
It looks like he's trying to heal it. So, I bet the bone's not dead. Since the nonunion didn't arise from a problem with the bone, I think the culprit must be the fixation. It wasn't rigid, so the bone didn't heal.
Adam Starr
Dallas, Texas
Date: Mon, 2 Jul 2001 21:27:54 +0600
From: Alexander Chelnokov
Hello Adam,
AS> I would replate it. Open it, remove the old hardware
I go your way to this point.
AS> debride
Why? It looks like hypertrophic non-union so no need to touch interfragmentary and periosteal tissues - stabilization is enough.
AS> and culture the wound.
Any sign of infection is happily absent.
AS> Then do your best to bring it out to the right length (maybe compare to films of the contralateral side)
Yes. The film is needed to estimate distal RU joint and to prepare the nail.
AS> and plate it again. I'd get 8 cortices on either side of the
Maybe our suggestion is more intuitive rather than gained from a well designed research but the closed nailing looks much less traumatic, stable enough, allowing early function and loading.
AS> It looks like he's trying to heal it. So, I bet the bone's not dead. Since the nonunion didn't arise from a problem with the bone, I think the culprit must be the fixation. It wasn't rigid, so the bone didn't heal.
In this statement i am completely with you again ;-)
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 2 Jul 2001 13:12:37 -0700
From: John Ruth
He needs to be replated with at least 6 cortices of purchase proximal and distal, bone graft optional as it appears to show trophic changes at the fractures site. It is clear that the nonunion is a result of inadequate fixation at the initial surgery. Does he have distal radio-ulnar joint symptoms? I cannot tell if the radius is short.
Date: Tue, 3 Jul 2001 08:51:16 +0600
From: Alexander Chelnokov
Hello John,
JR> fixation at the initial surgery. Does he have distal radio-ulnar joint symptoms? I cannot tell if the radius is short.
He has irradiating pain with motions, no pain in palpation above the RU juoint and obvious shortening of the radius comparatively to xrays of the contralateral forearm.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 3 Jul 2001 08:57:50 +0600
From: Alexander Chelnokov
Hello Dr. Krishnakumar,
DK> The inferior radio ulnar joint has subluxated because of shortening of the radius. This should also be taken in to account while planning treatment. My suggestion will be to remove the plate and distract the fracture using orthofix or Ilizarov. Bone grafting may be needed only if the fracture site
It is almost exactly what my plan is! I plan to apply a simple distractor using the Ilizarov set, then remove the plate, do slight tension to restore length of the radius, then perform closed nailing in the position. I suggest the traction will be like that we use to treat hypertrophic pseudarthroses, only tension stress, not a complete rupture of the site with gap formation.
Well, i'm going to the theatre for the surgery so keep fingers crossed please ;-)
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 3 Jul 2001 19:15:33 +0600
From: Alexander Chelnokov
Hello All,
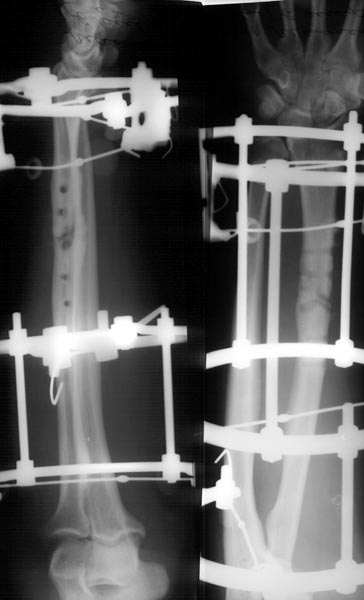
And in the end - result is what was suggested by Dr. Krishnakumar. Attempt to insert the nail failed - medullary canal was filled by bone. :((
Tissues under the plate were gray and black due to metallosis, so i just debrided the area, left interfragmentary tissue intact and applied circular ex-fix (x-rays attached) without grafting. This must be enough for the pattern of hypertrohic nonunion. After slight tension the distal RU joint looks OK. See attachment for the result of the surgery.
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 03 Jul 2001 09:34:02 -0500
From: Steven Rabin
I'd take out the failed hardware, culture it, bone graft, and replate it, but use more appropriate technique. I'd want at least 5-6 cortices on each side of the fracture, and I'd want to be sure that the screw crossing the fracture site it truly a lag screw. He needs mechanical stability to heal. Try to avoid periosteal striipping as you need to restore an appropriate biological environment as well. If it is infected, treat the infection with appropriate antibiotics. A rod would damage intramedullary blood supply at the same time you are damaging extramedullary blood supply while removing the plate.
Date: Tue, 03 Jul 2001 09:55:14 -0500
From: Steven Rabin
The external fixator seems like a whole lot of effort for what was probably a simple problem. The metallosis was from loose metal because there wasn't enough mechanical stability. Why go through all the effort of the fixator, when the surgery to remove the plate has already set exposed enough to rapidly apply another plate and be out of the O/R? Less risk from prolonged anesthesia time, less risk of damaging something important with the pins, less hassle for the patient taking care of his pin sites etc. If it was hypertrophic, he should heal with stability. Why do all this?
Date: Tue, 03 Jul 2001 09:10:27 -0400
From: Kevin Pugh
Sounds like a lot of work and equipment for what appears to be a very straightforward case.
kp
Date: Tue, 3 Jul 2001 23:09:45 +0600
From: Alexander Chelnokov
Hello Steven,
SR> The external fixator seems like a whole lot of effort
It was a shortest part of the surgery ;-) About 30 minutes with closed eyes.
SR> for what was probably a simple problem.
Hypertrophic nonunions - a classic indication to exteral fixation.
SR> Why go through all the effort of the fixator, when the surgery to remove the plate has already set exposed enough to rapidly apply another plate and be out of the O/R?
Because it would require at least skeletization for the plate. And graft harvesting from another area. And second surgery to remove the plate. And expecting a refracture after the removal.
SR> Less risk from prolonged anesthesia time,
No meaning - he takes for himself a local anesthetic which acts about 6-8 hrs. So when i visited him in the floor before leaving for home he still didn't feel any pain his forearm.
SR> less risk of damaging something important with the pins,
Ilizarov tehnique for the forearm is so well designed so it is literally equal to zero.
SR> less hassle for the patient taking care of his pin sites etc.
The meaningful point. But he is a physician, and he is from the city - so no problem to visit a clinic. He plans to return to work with the fixator in place yet.
SR> If it was hypertrophic, he should heal with stability. Why do all this?
To provide the stablity by less invasive measures.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 3 Jul 2001 14:48:31 -0700
From: John Ruth
This seems to be an example a treatment option that could be done and will likely work, but why torture the patient with an Ilizarov device when a simple plating with distraction to restore radial length with bone grafting of the defect would also likely work. You opened the fracture to remove the plate and screws. Why put the patient through the discomfort and pin site problems not to mention the potential for nerve or vessel injury during pin insertion.
Date: Tue, 3 Jul 2001 14:48:31 -0700
From: John Ruth
I would contend that the plate does not and should not be removed once the fracture has healed.
Date: Fri, 2 Jan 1998 20:47:18 +0530
From: Dr. Krishnakumar
Dear Dr Chelnokov,
I agree with all your points. This patient needs to have his distal radio ulnar joint addressed. The best way is to do it with external fixateur of your choice. I am not able to think of any other way to incease the length of the radius.
Dr.S.Krishna Kumar
KKOH
Overbridge, Parvathipuram
Nagercoil, Tamil Nadu,
India.
Date: Wed, 04 Jul 2001 09:49:38 +0000
From: b.meinhard
Actually the Ilizarov, although not a method with which most of the American surgeons are comfortable with, answers all of the problems inherent in this fracture problem and does so with one operation. For those most comfortable with this technique, Alex, a view of his sent X Rays shows that all issues will be solved. The best treatment is that which for the patient and the physician will give the most predictable results without, in their experience, causing major complications. It seems Alex's method burns no bridges.
BPM
Date: Wed, 4 Jul 2001 11:34:16 +0100
From: Nuno Craveiro Lopes
Dear Dr. Ruth,
You get one point, but, Why torture the patent with the possibility of graft site morbility, infection, a further intervention to remove material, site morbitity after removal, etc. if you can be sure that with Ilizarov this does not happen and you get a good result at first attempt?
I think that one must chose the method with those priorities: 1) The one that has the high probability to resolve the problem at first attempt with less complications. 2) The one with which one has experience enough to utilise it properly.
It seems Alex has made his choice right.
Best regards,
Nuno Craveiro Lopes
Almada, Portugal
Date: Wed, 4 Jul 2001 17:05:06 +0600
From: Alexander Chelnokov
Hello Nuno,
NCL> utilise it properly. It seems Alex has made his choice right.
I don't think any absolute answer about right or wrong exists for case like this. I in my particular environment weighted all circumstances including the mentioned by you and the arrow pointed to the way i used.
Anyway THX for the support. :-)
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 4 Jul 2001 09:38:18 -0400
From: Dr. Manuel Sotelo
Alexander
I have no idea how in your land the economical issue is managed. Is there a big differencein pricebetween a Ilizarov system an a plate? Does the patient pay for the implant or do you have a goverment stock in the hospital?
Regards
Manuel Sotelo
Date: Thu, 5 Jul 2001 00:03:21 +0600 From: Alexander Chelnokov
Hello Manuel,
DMS> I have no idea how in your land the economical issue is managed.
Frankly speaking me too.
DMS> Is there a big difference in price between a Ilizarov system an a plate?
In general no.
DMS> Does the patient pay for the implant or do you have a goverment stock in the hospital?
I work in a state institution so we must be reimbursed from the federal budget. But really the funding is much less than stated so there is a lot of activities of our senior management staff which can hardly be systematized. Some people must pay for all treatment, some for implants only, some not at all, some pay to insurance companies, some to implant trading companies, and so on, and they constantly change the rules.
Some implants like old fashion femoral nails and Ilizarov sets we have in stock so can use them for everybody for free, some are in deficience so different ways we use - keep asses of our administration kicked (little or no effect), request rich patients to buy implants not only for themselves but few extra ones, somtimes an insurance company pays the bill... I am not sure the situation can be realized clearly by colleagues abroad mostly because we ourself can not understand how surgeries are still performed yet.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 4 Jul 2001 12:41:43 -0700
From: John Ruth
I agree and have some experience with Ilizarov techniques (certainly less than you) and my first choice would have been internal fixation. I would not remove the plate and find that graft site morbidity is less in my hands than the problems with the Ilizarov (most of which are patient related). I find patients that I see very intolerant of the Ilizarov. Certainly in some situations it is not only the best but only alternative. If there are other alternatives which I feel will fix the fracture or nonunion then I always choose them first.
Date: Thu, 5 Jul 2001 08:55:29 +0600
From: Alexander Chelnokov
Hello John,
JR> than the problems with the Ilizarov (most of which are patient related).
This particular patient is more than compliant being a physician. He doesnt't have to leave for another city postperatively, like many our patient do, so we don't use the Ilizarov for them as we can't control it.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 5 Jul 2001 09:36:06 -0400
From: Dr. Manuel Sotelo
I am not sure the situation can be realized clearly by colleagues abroad mostly because we ourself can not understand how surgeries are still performed yet. I surely do. Except that the insurances companies paying to a hospital (even in private practice when they pay, they pay 6 to 8 months later..) the public hospital system works alike here.
Regards
Manuel Sotelo
Date: Mon, 20 Aug 2001 17:16
From: Bill Burman
Alex
About 6 weeks ago you presented this interesting case of an anesthesiology colleague with a failed plate fixation of a Galeazzi fx.
Instead of replating, an Ilizarov radio-ulnar ex-fix was selected.
It appears that the radio-ulnar fixator has locked the forearm in neutral rotation.
Most textbooks here recommend about 6 weeks of distal radio-ulnar joint immobilization by either casting or transarticular DRUJ pinnning in supination before restoration of forearm rotation. What is the plan to restore forearm rotation at this point? It seems that for an anesthesiologist - with all the knobs they have to twist - limited forearm rotation could be a problem.
Date: Mon, 20 Aug 2001 17:34:38 -0500
From: Steven Rabin
hi all
the forearm isn't moving and it doesn't look healed yet either. I'd suggest fixator removal and replating with bone graft then aggressive physical therapy to try to regain motion. I don't see a synostosis at this time, but continued cross radioulnar fixation could lead to that, and synostosis is very difficult to reliably treat.
obtain stable, even rigid, internal fixation and move it!
steve rabin
chief orthopaedic trauma
loyola
Date: Wed, 22 Aug 2001 16:28:51 +0600
From: Alexander Chelnokov
Hello Bill,
BB> Most textbooks here recommend about 6 weeks of distal radio-ulnar joint immobilization by either casting or transarticular DRUJ pinnning in supination before restoration of forearm rotation.
It looks like a superstition because practice doesn't prove this - in acute fractures 2-3 months, and even more long period of ex-fix doesn't lead to stiff restrictions of rotation. According to the forearm Ilizarov technique, immobilization should be in neutral position only with no care to an injury level. Even from common sense easier to restore 90 degrees from neutral position to both directions than 180 from supination to pronation.
BB>What is the plan to restore forearm rotation at this point?
He had almost full ROM preoperatively so I don't expect any trouble with this.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia