
Date: Wed, 25 Jul 2001 23:27:38 +0600
Subject: Femoral fracture with a rotated wedge
Hello all,
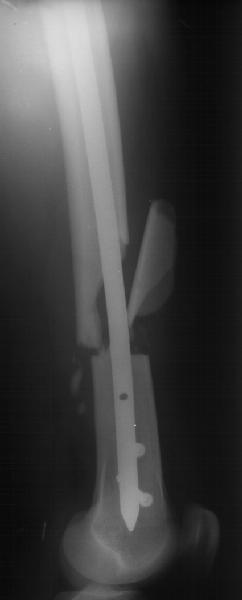
A male 19 years old admitted to us after a car accident (was inside) with this femoral fracture (see attachment). As you can see, there is a rotated fragment. The question is whether closed nailing "as is" and early knee function is enough for the case, or open reduction of the fragment should be performed?
|
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 25 Jul 2001 14:16:02 -0500
From: Adam Starr
Hi Alex.
I would treat this with a reamed, statically locked nail, using a closed technique.
Would I try to spin that butterfly fragment around? I don't know. There are plenty of pictures in textbooks that show exuberant callus formation around comminuted, poorly aligned fragments. I think it would heal as is.
According to a study done by R. Brumback, static locking with one proximal oblique screw and two distal transverse screws will be stout enough to allow immediate full weight bearing (as long as the screws are at least 6mm diameter), even if the comminution is so severe that there's no cortical contact.
Would it hurt to make a tiny stab wound to spin that fragment into a better position? I don't know. It probably wouldn't. But I think you'd be treating the Xray if you do that. I think this fracture will heal just fine if you nail it.
Adam Starr
Dallas, Texas
Date: Thu, 26 Jul 2001 02:00:10 +0600
From: Alexander Chelnokov
Hello Adam,
THX for your comment!
AS> I would treat this with a reamed, statically locked nail, using a closed technique.
This is the option i prone to (but unreamed, we have no flexible reamers).
AS> the screws are at least 6mm diameter), even if the comminution is so severe that there's no cortical contact.
At the moment 4,5 cortical lag screws can be used. Locked nails are prepared from conventional solid titanium ones with 5 mm holes drilled.
AS> you'd be treating the Xray if you do that. I think this fracture will heal just fine if you nail it.
How about m.quadriceps function - will the fragment interfere with its sliding?
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 25 Jul 2001 15:09:47 -0500
From: Adam Starr
How about m.quadriceps function - will the fragment interfere with its sliding?
I doubt it. I would treat it closed, but there may be folks out there who'd disagree.
Adam
Date: Thu, 26 Jul 2001 03:02:06 +0000
From: b.meinhard
I would nail the femur with a static rod and I would not worry about the fragment. It will incorporate. Of course a better X Ray would result with a mini open procedure.
BPM
Date: Thu, 26 Jul 2001 00:57
From: Bill Burman
If Alex could ream, could the fragment be flipped with an intramedullary hook?
Date: Sat, 28 Jul 2001 23:45:49 +0530
From: Dr. Krishna Kumar
Dear Dr,
Just have a look at the attached X-rays. The patient had ipsilateral tibial fracture also which was also nailed and locked. The pre operative X.ray was taken in Jan 2001 and the other two x rays were taken in July 2001. These fractures were close nailed.
 |
 |
 |
Dr.S.Krishna Kumar
KKOH
Overbridge,
Parvathipuram, Nagercoil
Tamil Nadu, India
Date: Tue, 31 Jul 2001 20:28:42 +0600
From: Alexander Chelnokov
Hello All,
THX for all suggestions and wonderful clinical cases. I just performed closed nailing with static locking. Images attached. We still haven't yet availavble thick locking bolts so use 4,5 cortical screws instead so i don't plan to hurry with weight bearing. Comments are welcome.
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 31 Jul 2001 03:32:01 -0400
From: bruce meinhard
Agree with delayed weightbearing. Bucholtz wrote an article with reference to distal femur fractures within 5 cm. of the proximal of the two distal locking holes...50% of the intact femur strength was necessary by healing to prevent a fracture through the nail at the level of the hole in the rod.
bpm
Date: Wed, 1 Aug 2001 23:54:20 +0600
From: Alexander Chelnokov
Hello All,
A propos to the case - i am curious does OTA/AO fracture calssification reflect the feature of the discussed wedge fracture? Does the pattern have the same coding as a fracture with the a non-displaced butterfly fragment?
I would greatly appreciate if you share your experience what is necessary after closed femoral nailing. I mean what routine measures like antibiotics, anticoagulants, compressive devices, continuious passive motions etc should be used and how long. I mean pure cases, not mixed with other severe injuries. Say, single femoral shaft fractures in young adults without any pre-existing health problems. THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 06 Aug 2001 12:10:33 -0600
From: Thomas A. DeCoster
Regarding OTA Classification of fractures.
The shaft segment of long bones is subclassified into types by degree of comminution (although AO doesn't like the English word comminution).. A is no comminution (2 fracture fragments "simple") B is comminuted ("complex") (3 main fracture fragments or the presence of a "wedge" fragment. C is segmental comminution (another "complex") where the main proximal fragment is not in contact with the main distal fragment when reduction is present. Neither AO nor OTA classifications include displacement of fractures (or malrotation as in your case) as a significant consideration in classification; even down to groups and subgroups.
This shortcoming is at least partially justified by the inability to accurately measure and report displacement, angulation and the like. It is NOT to say that such fracture characteristics are not clinically important.
Winquist classified femur shaft fractures by degree of comminution but the importance and usefulness of this classification was greatest before locking nails. It's not terribly useful or important now with routine use of locking nails.
Routine postop protocol for patients with isolated femoral shaft fracture treated by intramedullary nail would include perioperative antibiotics for 48 hours, Ace wrap compressive dressing to the limb for swelling control, immediate ambulation with crutches with partial weight bearing advancing to full over 2 months and active assisted range of motion to the hip and knee. Individual problems addressed as needed but most patients do very well with this general approach.
td