

Date: Wed, 5 Sep 2001 23:09:09 +0600
Subject: Ipsilateral acetabular, femoral neck and shaft fractures
Hello all,
A 23 y.o. male after a car accident transferred to us from elsewhere at 4th day since the injury. He has the pelvic ring lesion including fracture of the left acetabulum, and ipsilateral femoral neck and shaft fractures - images attached. The shaft fracture is open grade II, debrided at the initial hospital - no sign of infection to date.
Our plan is to apply an external fixator with femoral extension, and maybe percutaneous fixation of the acetabulum. And some days later if no infection and patient is in stable condition - closed nailing of the shaft, lag screws for the neck. Your comments and suggestions are welcome.
|
|
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 05 Sep 2001 12:58:54 -0500
From: Adam Starr
Hi Alex,
Closed or limited open reduction and percutaneous screw fixation of displaced acetabular fractures is hard. Getting the right image views is hard (you have to have an excellent fluoro technician), and placing the screws safely is hard (you have to know which views to look at to be sure you're safe, and how to hit a small target with your screws). Reducing the fracture adequately is hard, too. It's even harder if you wait more than a couple days.
Reduction is going to be critical to success in this young man, because his fracture looks like it goes pretty high in his dome. Do you have Judet views and a CT scan you can show us?
Depending on his acetabular fracture pattern...I think I would probably chose a recon nail to stabilize the femoral neck and shaft with one implant, and fix the acetabular fracture through a Kocher - Langenbeck incision. The nail could be placed through that approach, and you'd be able to reduce and fix the neck fracture, too. A single 6.5 screw placed anterior in the neck is helpful to stabilize the neck fracture while the recon nail screws are going up into the femoral head.
I would also repair his pubic rami fractures. But there are lots of people in the US who think that's a bunch of hooey. You're going to have to reduce his right ramus fracture as part of your acetabular fracture reduction, I think. It looks like it needs to be rolloed forward and laterally. The left sided rami have been pushed inard - you'll need to draw them out to fix them. I can't tell if his superior and inferior rami are separate on these views. There may be a bridge of bone connecting them, but I can't tell if it's solid or not. If they are separate, then you'll need to approach him from front and back to be able to control all the parts of his T shaped fracture.
Good luck.
Adam Starr
Dallas, Texas
Date: Thu, 06 Sep 2001 07:35:00 -0700
From: Chip Routt
Hello Alex-
It is impossible to discuss such a complex patient situation based on AP femur and pelvic plain radiographs together.
Chip
Date: Thu, 6 Sep 2001 23:02:03 +0600
From: Alexander Chelnokov
Hello Adam,
AS> because his fracture looks like it goes pretty high in his dome. Do you have Judet views and a CT scan you can show us?
I found inlet and one Judet view. CT is not available - the CT machine is in another building. In the next message i attached three views in external fixator.
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Fri, 7 Sep 2001 02:22:33 +0600
From: Alexander Chelnokov
Hello Chip,
CR> It is impossible to discuss such a complex patient situation based on AP femur and pelvic plain radiographs together.
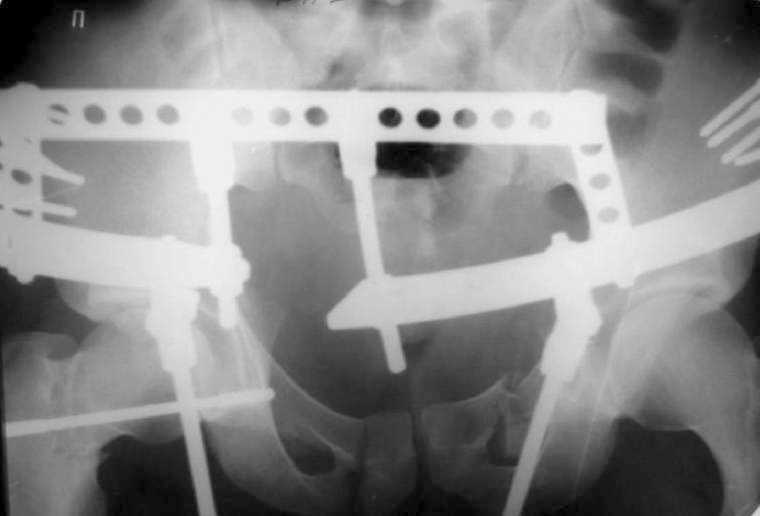
See attachment for AP and Judet views after external fixation. Our pelvic guys tried to reduce the acetabulum with the transarticular pin inserted through the lower part of the head. They are satisfied with the pattern and plan to insert a percutaneous screw to fix the position during a surgery for the neck and shaft fracures.
 |
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 06 Sep 2001 13:38:48 -0700
From: Chip Routt
wow
Date: Fri, 7 Sep 2001 20:22:35 EDT
From: Cory Collinge
Alex-
Had this young man come to me the night of his injury I would have:
If the patient came in at 4 days (as he did to you). My first priority (assuming the thigh wound was clean) would still be the femoral neck, followed closely by the acetabulum and then the femoral shaft. I would:
Personally, I have and will continue to avoid transarticular acetabular pins under almost any circumstances. They can bend or break, and really aren't necessary if the fractures get fixed in a timely manner. I have similar thoughts re: hip spanning ex fix.
Cory Collinge
Ft. Worth, TX
Date: Fri, 07 Sep 2001 18:04:25 -0700
From: Chip Routt
No problem then.
I remain impressed/amazed/stunned/saddened how anyone can recommend definitive treatment actions for this patient with absolutely incomplete radiographic and clinical information.
This complex patient's best chance for success is in the plan, which is based on the details, which we don't have.
Pretend that this patient is in your ER - do you perform your written recommended treatments without additional info? How do you grade the resident or student that presents this patient to you with this incomplete info and embarks upon treatment plans?
Imagine if you are this patient - and your surgeon is treating you based on advice, based on incomplete data, from an American stranger with a computer.
We can offer this - proper wound management using appropriate surgical debridement, tetanus prophylaxis, systemic (and perhaps local) antibiotics, nutritional support, skeletal stability after accurate fracture reduction, appropriately timed/sequenced operative intervention(s), and patient & his joints mobilizations.
No need to be sorry.
God Bless Texas-
Chip
Date: Sat, 8 Sep 2001 10:04:03 +0600
From: Alexander Chelnokov
Hello Cory,
Cac> Personally, I have and will continue to avoid transarticular acetabular pins under almost any circumstances. They can bend or break
This pin has been applied for reduction and provisional fixation and is to be removed immediately after definitive stabilization.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sun, 09 Sep 2001 09:24:47 -0500
From: Adam Starr
Alex,
It's still hard for me to see the acetabular fx clearly due to the ex-fix hardware.
If they go ahead and fix it, be sure to try to post some good images for us, so we can see what sort of reduction they accepted.
Adam
Date: Sun, 09 Sep 2001 10:05:37 -0500
From: Adam Starr
Hi Cory,
The repair of pubic rami fractures is an interesting question. Might be fun to talk about. Alex's case is so complex, with so many issues to argue about...maybe pubic ramus fractures are less contentious.
I know Joel Matta reports good results with non-operative management of sup pubic ramus fractures. Kyle Dickson reports the same thing. I think they tend to repair the ramus fractures if they're markedly displaced - I'll have to pull Kyle's article to see exactly what he said. Paul Tornetta's article written with Matta also discusses this point. I think the idea is that the inguinal ligament is stout enough to prevent displacement. Hopefully Kyle will comment on this - I'm sure I'm misquoting his study.
(I wonder about our ability to predict the competency of a ligament on the basis of a plain Xray. The old question, where were the fracture ends at the moment of the injury? makes me wonder if those "minimally displaced" pubic ramus fractures could really be completely unstable injuries in disguise...)
I seem to remember Marvin Tile discussing pelvic ring stability at his course in Toronto (a great course, by the way - I recommend it highly) and saying that the anterior ring accounts for something like 40% of the ring's resistance to vertical displacement. Again, I don't have the study at hand, and I'm probably misquoting. But, the gist of it was that the anterior ring counts for something as far as stability goes. God gave you an anterior pelvic ring for a reason.
I'm pretty sure Chip Routt has done biomechanical studies comparing fixation in the back only to fixation in front and back, but I can't recall if the anterior injury he looked at was a symphysis diastasis (everyone seems to have no trouble fixing those) or a ramus fracture.
Most everybody says you should fix symphysis pubis disruptions, if they're wide enough. I guess you can quibble with the exact measure - would anybody balk at ORIF'ing one that was greater than 2.5cm wide? That's what Dr. Tile's book recommends. (His book also recommends fixing ramus fractures in type C ring injuries).
A small pfannenstiel to plate a symphysis diastasis is a pretty simple approach. I wonder if the simplicity of the approach has anything to do with the fact that so many people recommend repair of symphsis injuries? Plating a ramus fracture is a little bit bigger deal, especially if the fracture is a high one, out near the pecten - maybe the extra dissection is what makes people shy away from it? Are fans of the stoppa approach more likely to fix ramus fractures?
If you can repair a ramus fracture, and thus gain improved stability, and you can fix it with very little morbidity, shouldn't you go ahead and fix it?
Adam Starr
Dallas, Texas
Date: Mon, 10 Sep 2001 20:16:31 +0600
From: Alexander Chelnokov
Hello Adam,
AS> It's still hard for me to see the acetabular fx clearly due to the ex-fix hardware.
Maybe you'll get accustomed sooner or later :-)
AS> If they go ahead and fix it, be sure to try to post some good images for us, so we can see what sort of reduction they accepted.
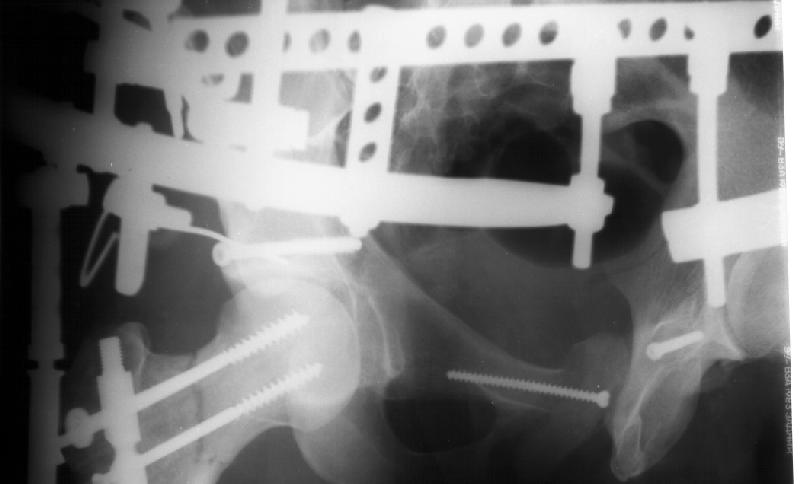
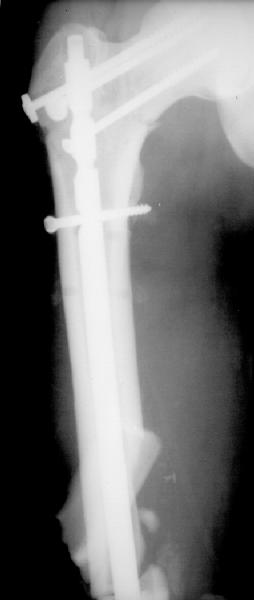
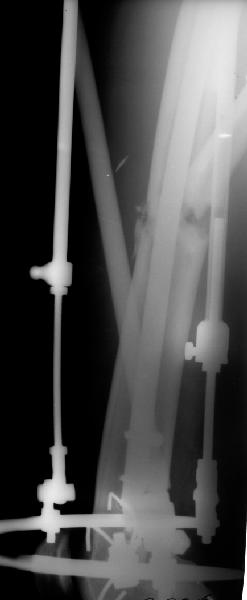
OK, we just fixed all fractures as the patient shows no infection signs. Posterior column was perQ (nice abbreviation) fixed by a screw and a wire, rami - by screws. Then closed locked nailing was performed (i placed a single screw at the upper level - is it commonly acceptable?) and "miss a nail" three cancellous screws to the neck (at the moment we have no more available implants suitable for this lesion like gamma nail etc, so the choice was easy :-). The external fixator left in place as a "local sceletal traction" for a couple of weeks. Acetabular, femoral shaft and neck images attached.
 |
 |
 |
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia