
Date: Sun, 19 May 2002 15:21:58 +0600
Subject: Elbow instability
Hello All,
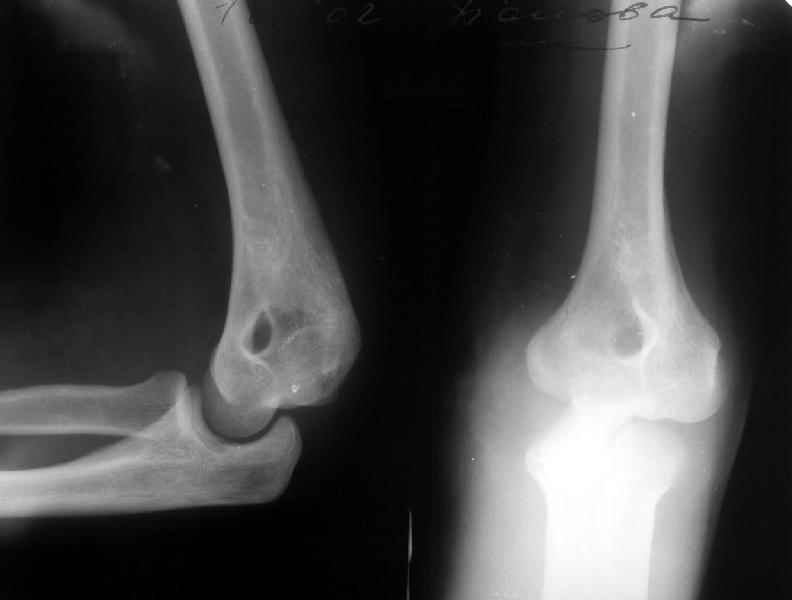
A female 48 years old sustained multiple injuries after fall from 5th floor 28/04/02. Among other injuries there was open posterior elbow dislocation (see attachment). It was reduced and the wound at the medial side of the joint debrided at the initial hospital. May 7 she was transferred to us. The wound healed primarily.
|
Yesterday (3 weeks post reduction) the plaster was removed to start motions. Gross elbow instability was revealed - the forearm easily can be displaced medially, and reduced back. Recent films with and without subluxation also attached.
 |
 |
What to do? Continue plaster for some more weeks? Revision and repair of medial collateral ligament? XF with hinges? Today the elbow ROM is about 60/150 (with 180 as full extension).
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sun, 19 May 2002 19:09:06 +0100
From: chris wilson
Our elbow specialist recommends open reconstruction of the MCL of the elbow, and protection with a hinged elbow fixator. He recommends a fixator made by Stratec, named after Mr Morey from the U.S.
Date: Mon, 20 May 2002 07:52:27 -0400
From: James Carr
I agree with Chris. I would approach the elbow medially if it appeared primary medial instability. If it is true "global", needing some lateral work as well, everything can readily be reached by posterolateral approach next to olecranon. Be ready to do graft if needed medially. For the few cases I have used them, elbow fixators have worked well. I think EBI has one too.
Jim Carr
James B. Carr, MD
Palmetto Health Orthopedics
Date: Mon, 20 May 2002 14:00:52 -0600
From: Thomas A. DeCoster
For recurrent elbow dislocation I suggest:
1. Scrutinize the radiograph carefully for avulsion fractures and repair them.
2. Assess for tendon avulsion.
3. Exam under anesthesion with assessment of MCL and LCL
4. Document stable ROM after initial reduction and try to stay within that range postop. Presumably this was done and the patient still re-dislocated. So repair the ligaments that are torn.
5. Medially there are 3 components but the anterior band is most important and is usually torn from the humerus. Reattach it with drill holes or suture anchor.
6. Laterally there are 4 components with the lateral humeral-ulna most important; again usually avulsed as a sleeve from the humerus and reattach the whole complex with drill holes or suture anchor.
7. If still unstable then articulated XF. Olganesen had a ring frame decades ago.
8. Commonly fractures participate in the instability(avulsions, proximal radius, coronoid, olecranon,...) and need fixation; although not apparant in your case.
Tom DeCoster
{kind=link}