

Date: Wed, 9 Jul 2003 19:45:03 +0600
Subject: THA after multiple injuries
Dear All,
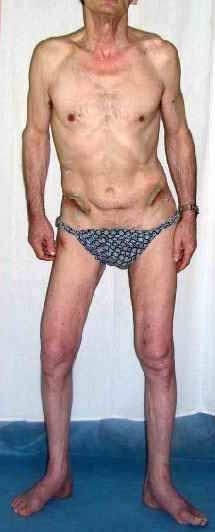
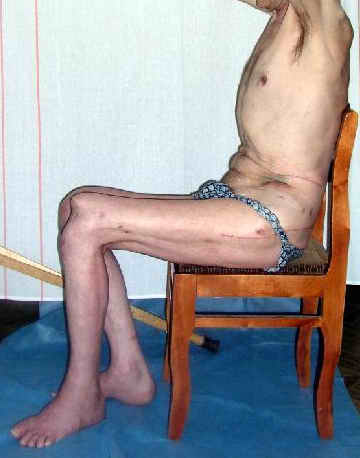
A male 53 years old Nov. 25, 2002 sustained multiple injuries including pelvic ring lesion, # of the left acetabulum, # of the right femoral shaft, left patella, also left ankle and right forearm. He was initially treated elsewhere on traction, the ankle in plastre cast and the forearm with ex-fix.
Referenced to us Mar. 25, 2003 - 4 months after the injury with healed femur, ankle and forearm. Pelvic external fixator was applied to correct the ring shape. Apr 28, 2003 the symphisys was plated and acetabular ORIF was performed mostly to prepare it for later THA.
Now he walks with crutches, with pain in affected hip, radiologic changes of the head are in progress. In other words the joint is ready for replacement.
However there are some features: at the same side there is deficiency of the patellar tendon with the patella fixed to the femur, and active knee extension is absent.
|
|
|
|
At the opposite side (right) there is femoral malunion, lack of full knee extension though the extremity is weight-bearable. Shortening is 3 cm.
So questions are - what to do with the left patella and quadriceps at the side of THA? Should axis and length of the opposite (right) femur be restored before? If not to touch the right femur, should the left femur be shortened during the THA?
X-rays attached.
 |
 |
 |
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 9 Jul 2003 14:39:41 -0600
From: Terry Finlayson
Tough case!
1. I would take down right femur nonunion and correct translation (it looks at very high risk to refracture), shortening and mild flexion deformity (these latter two corrections look like they would gain at least 1 cm of length.
2. Explore left knee/extensor mechanism. If adequate patellar tendon/ quad tendon integrity and at least 60 degrees arc of motion (including full extension), I would attempt extensor mechanism repair/reconstruction (the specifics would depend on the exact findings). If repair/reconstruction not feasible or ROM too limited I would proceed to knee arthrodesis, at which time 1-2 cm shortening of left side could be done.
3. Left THA can be done, but I wouldn't try to shorten very much at THA site because he's already short due to protrusio (compare levels of lesser trochanters to your reference of choice on the pelvis) and any significant shortening at hip may lead to poor abductor tension and attendant risk of dislocation (offset stem and liner options may allow correction for these).
4. If left hip pain is main problem, I would consider doing all left extremity procedures initially; however, I'd be concerned about that malunion on the right absorbing more loading.
Terry I. Finlayson, M.D.
Alpine Orthopaedic Specialists
North Logan, UT 84341
Date: Thu, 10 Jul 2003 01:10:24 EDT
Subject: Re: [1/2] THA after multiple injuries
Hello:
I would not address the healed distal femur on the right. Leave it alone for now.
I would, I think, manipulate the left knee (expect little improvment but maybe one is surprised), total hip on left. Since right is short, shorten the left during the total hip as one can without compromise of the implant and the add lift to other sided as needed.
Good luck.
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005