
Date: Thu, 18 Dec 2003 03:31:56 +0500
From: Alexander Chelnokov
Subject: Unhappy (valgus) tibia nailing
Dear colleagues,
A female 24 years old, a sister of a friend of mine (not physician) living in Moscow, 3 weeks ago admitted to the hospital in Moscow after a car accident (was a pedestrian) with a tibial shaft fracture. 3 days ago closed locked nailing was performed, see attached films. Now he is in panic because they are going to remove the nail and perform plating.
It seems to me the situation can be solved on the current nail with a minimal procedure - insertion of wires into distal and proximal tibia, acute distraction and proximal static locking. Maybe dynamic locking screw should also be removed before. As a maximum i would assume to pull the nail to the central fragment, insert poller wire or screw, then insert of the nail back and lock it.
|
Any suggestions? THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 17 Dec 2003 18:50 EST
From: Bill Burman
Alex
Bob Winquist gives a good OTA Basic Fx course talk on how to avoid valgus nailing of proximal tibial fractures with much emphasis on starting point
Date: Wed, 17 Dec 2003 23:41:06 EST
From: Tadabq
The tibia shaft fracture (proximal 1/3 of the shaft) is apex medial 20 degrees, slightly short and a few degrees apex anterior after nailing. The nail extends quite proximal to the entry site. I wasn't able to see the distal end of the nail on my screen and am not certain if there was distal locking.
There are many techniques to try to avoid this problem and some to correct it once it happens. Correction seems harder than prevention and has always been harder than I anticipated when going back in. If you back the nail up, reduce the fracture and re-insert the nail then the deformity has a strong tendency to recur. Extracting the nail and plating is not altogether unreasonable, although I would prefer to reposition the nail.
My best salvage technique (2 cases) has been
in the first case I left the two hole plate and in the second I removed it at the end of the case. Both turned out ok.
Poller or blocking screws (or as you suggest wire?) CAN also work but once the channel in the proximal fragment is created it can be difficult to maintain the reduction while the nail goes back in.
Patience and good positioning and radiographic visualization are helpful.
Very salvageable.
Tom DeCoster
Date: Thu, 18 Dec 2003 07:41:23 -0500
From: James Carr
Good ideas Tom. Basically, it needs a shorter nail with a more lateral starting point. I once had a resident's case I was called into the middle of with the same problem occurring. I took the nail out, enlarged the incision to visualize the starting point, and lateralized the starting point considerably. I was amazed at how the valgus disappeared as I moved it laterally (it took a few tries- each one improving the valgus as I moved the starting point more lateral). Poller screws, and a nail without such a proximal bend are also good adjuncts. Also, the valgus won't correct unless you use a shorter nail that can be buried some- otherwise it impinges on the proximal entry cortex, and pushes it into valgus. In fact, during nail insertion, the tibia will continue to deform until the nail is fully buried.
Jim Carr
Date: Thu, 18 Dec 2003 21:09:12 +0530
From: Vineesh Mathur
Dear Alex,
I have simple technique for this particular problem. Reinsert the nail from a point in the proximal tibia exactly in line with the tibial crest . It is inevitably lateral but it saves the bother of trying again and again.
Best of luck,
Dr Vineesh Mathur
Sr. Consultant Orthopaedics,
Kalyani Hospital, Gurgaon, India 122001
Date: Thu, 18 Dec 2003 22:52:11 +0500
From: Alexander Chelnokov
Hello Bill,
BB> Bob Winquist gives a good OTA Basic Fx course talk on how to avoid valgus nailing of proximal tibial fractures with much emphasis on starting point -
THX for the good source. We use an "alternative" technique - a small wire distractor which allows to avoid this problem rather easily (image attached). And i guess it could help in the case but the patient is far from here.
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Fri, 19 Dec 2003 05:36:30 -0600
From: Obremskey, William T
These can be challenging. I agree w/ all Dr. Carr's points. My preference to prevent the deformity is to use an anteromedial plate. See attached case.
 |
 |
Bill
William T Obremskey MD MPH
Vanderbilt University
Orthopedic Trauma Division
131MCS 2100 Pierce Ave
Nashville, TN 37232-3450
Date: Fri, 19 Dec 2003 17:19:43 +0500
From: Alexander Chelnokov
Dear Bill,
OWT> These can be challenging. I agree w/ all Dr. Carr's points. My preference to prevent the deformity is to use an anteromedial plate.
Do you suppose reduction by temporary external fixator is less successful or more harmful/risky than site opening and plate placement? How dynamization here is performed if necessary?
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Fri, 19 Dec 2003 08:47:22 -0600
From: Obremskey, William T
The temporary ex fix is a good idea. I have used it for shaft fxs when an assistant is not available. I think it would be more difficult to control the proximal fragment intra and post op w/ a temporary fixator of any kind w/ these proximal fxs. Surgeons in North America are also in general less familiar w/ thin wire fixators. Healing has not been a problem in these proximal metaphyseal fxs and dynamization not necessary. Dynamization could also be done in the segmental shaft component if needed.
Bill
Date: Sat, 20 Dec 2003 13:48:18 +0500
From: Alexander Chelnokov Hello William,
OWT> The temporary ex fix is a good idea. I have used it for
shaft fxs when an assistant is not available.
Yes, sterile team can include only a surgeon and a nurse.
OWT> I think it would be more difficult to control the proximal
fragment intra and post op w/ a temporary fixator of any kind w/
these proximal fxs.
I mean ex fix only intraoperatively, post op alignment is kept by the
nail and locking screws. A poller screw(s) can be also added after nail
insertion prior fixator removal if any doubts.
OWT> Surgeons in North America are also in general less familiar w/
thin wire fixators.
:-) I think it was so 10-15 years ago because to date there is a lot of
highest quality papers on the topic from North America.
OWT> metaphyseal fxs and dynamization not necessary. Dynamization
could also be done in the segmental shaft component if needed.
The plate still remains a splint preventing axial compression. Of
course i don't have any proves that this is crucial in the particular
circumstances.
Best regards,
Alexander N. Chelnokov
Date: Mon, 21 Dec 2009 09:31:34 +0530
From: sathisv
Dear Dr Alex,
Thank you very much for presenting this case. The discussion following it
very informative
Will not the wires of this Exfix interfere with reaming and nailing ?
Dr Sathis Chandran
Date: Sun, 21 Dec 2003 23:26:09 +0500
From: Alexander Chelnokov
Hello sathisv,
Monday, December 21, 2009, 9:01:34 AM, you wrote:
s> Will not the wires of this Exfix interfere with reaming and nailing ?
The proximal wire is behind the nail, the distal one is lower.
Best regards,
Alexander N. Chelnokov
Date: Wed, 23 Jun 2004 21:28:05 +0600
From: Alexander Chelnokov
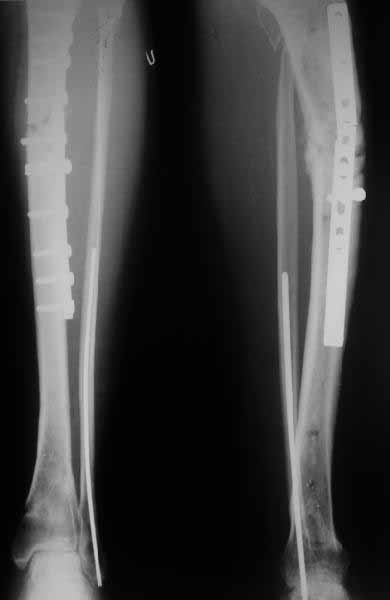
A> Some feedback regarding the case discussed here 6 month ago
I attached images with the nail (Dec 2003) and today with the broken
plate. The fracture site is pretty mobile.
We plan to remove the plate and perform closed nailng.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia

Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia