Date: Thu, 18 Dec 2003 03:31:56 +0500
From: Alexander Chelnokov
Subject: Supracondylar Femur Fx - Peri-Implant
Hello All,
Merry Xmas!!!
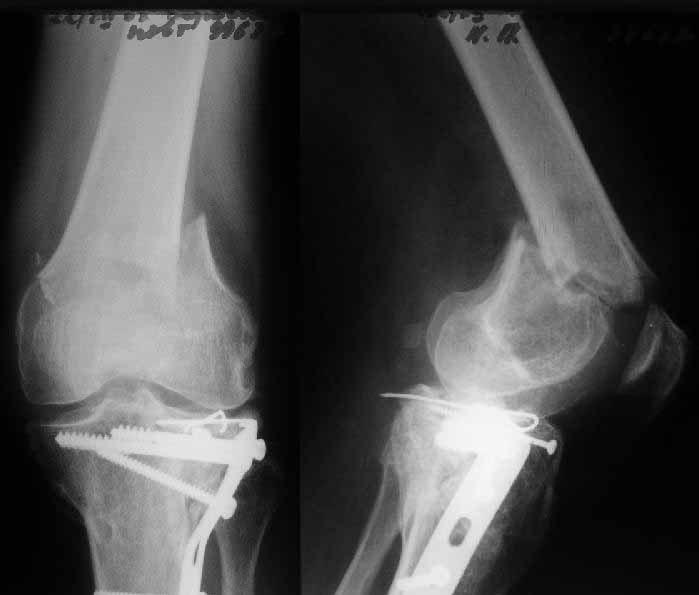
A male 52 years old was treated 1.5 years ago in our unit - ORIF of the proximal tibia. In 1 year follow-up all was OK - flexion 130, full WB, returned to work (white collar).
Two days ago he fell on a slippery sidewalk - x-rays attached. How would you manage the injury? My first thought is closed nailing. And more common question - what we should do routinely with posttraumatic local osteoporosis? When full WB and function of the extremity is restored how long does a problem of such fractures exist?
|
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 24 Dec 2003 17:50:05 +0100
From: J.C. Goslings
Hello Alexander,
Nailing seems a good option. We probably would use a Synthes LISS plate but I expect that this is not available in your hospital.
Good luck,
Carel Goslings
Trauma Unit AMC Amsterdam
Date: Wed, 24 Dec 2003 11:01:53 -0700
From: John T. Ruth
Many options for this. Would favor peri-locking plate if available, second choice blade plate, and last would be retrograde rod. Low fracture line and osteopenia makes retrograde rod last choice due to poor fixation of locking screws. Don't know answers to other questions. Certainly important though.
Date: Wed, 24 Dec 2003 21:59:30 -0600
From: Obremskey, William T
LISS plate, retro IMN, blade plate, or LCP. All would work. Are you sure it is not pathologic?
Bill
Date: Thu, 25 Dec 2003 09:15:46 +0500
From: Alexander Chelnokov
Hello John,
JTR> poor fixation of locking screws. Don't know answers to other questions. Certainly important though.
Maybe biphosphonates/somatotropin/etc should be administered for prevention of such fractures? Pharmacological companies would like the idea, wouldn't they?...
Hello William,
OWT> LISS plate, retro IMN, blade plate, or LCP. All would work.
I plan antegrade nail today.
OWT> Are you sure it is not pathologic?
If you mean tumor lesion it doesn't look like that.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 25 Dec 2003 18:54:10 -0800
From: Muhammad Amin Chinoy
I plan antegrade nail today.
i would have thought a Retrograde nail to be a better idea, though personally i would go for a DCS
M. Amin Chinoy
Date: Thu, 25 Dec 2003 18:39:09 EST
From: Tadabq
In this case a 52 year old male sustained a distal femur (supracondylar) fracture 1.5 years after plate treatment of a proximal tibia fracture which appearantly healed well. Apparently this was a low energy trauma and Alex suggests post traumatic osteopenia of the limb as a contributing or causative factor. In addition to the question of how to treat this individual patient, he poses the question how common is post-traumatic regional osteoporosis and how should it be treated or prevented and specifically is there a role for bisphosponates or somatotropins?
I'm not certain this patient has that condition but it seems logical. I'm not certain how to make the diagnosis. I would think 100% of patients have the phenomena of post-fracture osteoporosis to some degree, so the matter of defining the degree to which it causes clinical problems would be desirable. I would think the incidence of a distal femur fracture after a plated proximal tibia fracture is in the realm of 1/1000. That's probably the same rate for other parts of the body (fracture of an adjacent bone months after an initial fracture.) I would think the incidence would be less after operative treatment than after non-operative treatment, so perhaps there is some historical information available on this topic. I think mobilizing the patient as soon as possible with progressive return to normal activities would be the usual scenario and perhaps watch for the occasional patient with radiographic signs of more extreme forms of regional osteoporosis and diagnose and treat those somewhat more aggressively.
TD
Date: Fri, 26 Dec 2003 11:06:31 +0500
From: Alexander Chelnokov
Hello Tom,
TAC> I think mobilizing the patient as soon as possible with progressive return to normal activities would be the usual scenario and perhaps watch for the occasional patient with radiographic signs of more extreme forms of regional osteoporosis and diagnose and treat those somewhat more aggressively.
THX for the valuable reply. I suggest early mobilization and return to noramal activity already is the conventional scenario. In other words we should suggest such fractures not preventable? I am not certain where the border of more extreme forms of regional osteoporosis lies, and what is the optimal program if one suggests the local ostepenia is beyond the border.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Fri, 26 Dec 2003 16:34:19 +0500
From: Alexander Chelnokov
Hello John,
JTR> Many options for this. Would favor peri-locking plate if available, second choice blade plate, and last would be retrograde rod.
Why antegrade nail is not mentioned?
JTR> Low fracture line and osteopenia makes retrograde rod last JTR> choice due to poor fixation of locking screws.
I inserted 3 locking screws. Locking plates are still not available in our settings. Is there any comprartive study of locked plates vs nails in distal femoral fractures?
JTR> Don't know answers to other questions. Certainly important
Noted.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Fri, 26 Dec 2003 8:27 EST
From: Bill Burman
>Is there any comprartive study of locked plates vs nails in distal femoral fractures?
Date: Fri, 26 Dec 2003 15:19:12 EST
From: Tadabq
I don't know how to prevent them but that is not to say that they are not preventable. A good place to start looking would be the ones at highest risk, but I'm not certain how to identify them.
TD
Date: Sat, 27 Dec 2003 16:44:58 +0500
From: Alexander Chelnokov
Hello V,
VMI> I was thinking of a retrograde nail because I thought the fracture was too low. I would love to see the postop Xrays.
Sorry but I've just prepared postop images - attached. A solid 13 mm nail was used. A few degrees of recurvation appears to be which i missed on image intensifier.
 |
I'm still uncertain about advantages/disadvantages of ante/retrograde nailing for such fractures.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 1 Jan 2004 21:49:46 EST
From: Tadabq
the postop radiographs look excellent. What do people think about driving an antegrade nail this distal as compared to retrograde nailing?
TD
Date: Fri, 2 Jan 2004 09:06:39 -0000
From: Chris Wilson
Because retrograde nails are not without their problems. There's a poor choice of sizes, and you have to breach a normal joint, with risk of infection, and even greater risk of fat pad or patella tendon fibrosis later.
Regards
Chris Wilson
UIniversity Hospital
Cardiff UK
Date: Fri, 2 Jan 2004 10:55:22 EST
From: Tadabq
Those are all the arguments against retrograde nailing (surgical injury tothe knee), but there are advantages like better distal fixation and control. The antegrade nail in the case shown is probably into the knee joint slightly. This case looks great but there must be some risk of splitting the condyles or other knee joint injury when driving an antegrade nail this distal. The antegrade nail also has entry site problems including variable injury to the hip muscles, heterotopic ossification, femoral neck fracture, and positioning difficulties. Overall the entry site problems seem about the same for the two techniques. If that is the case then the decision might come down to which one offers better distal fixation and that might be retrograde nail. If there are more entry site problems with retrograde nail than antegrade the antegrade nailing might be preferable even if the distal fixation isn't quite as good or reliable. So, to me, it is a trade-off between benefits and risks for specific fracture patterns. Inthis case of a very distal femur shaft fracture the antegrade nail driven very distal in the femur looks extremely good. Without a comparative series we are left to base decisions on general principles, theory and related experience.
TD
Date: Sun, 4 Jan 2004 14:22:23 +0500
From: Alexander Chelnokov Hello Tom,
TD> the knee), but there are advantages like better distal fixation and control.
This strongly depends on a particular nail design - number of holes,
distance between them, distance from the distal tip of the nail to the
most distal hole. The latter distance can be minimized in antegrade
nail to literally 3-4 mm while retrograde nails have to reserve more
space for the threaded canal of the nail connecting screw.
TD> The antegrade nail in the case shown is probably into the knee joint slightly.
Not in this case. Though i have a couple of similar cases with 3-4 mm
prominence of the nail - looks asymptomatic or covering by pre-existing problems.
TD> This case looks great but there must be some risk of splitting the condyles or
other knee joint injury when driving an antegrade nail this distal.
The risk is minimized by using of a distractor with some olive wires.
Also canal in the condyles can be prepared by a long awl or covering
by pre-existisng problems.
TD> difficulties. Overall the entry site problems seem about the same for the two
techniques.
Isn't early knee mobilization easier without a recent local wound?
TD>If that is the case then the decision might come down to which one
offers better distal fixation and that might be retrograde nail.
Why retrograde nails offer better distal fixaton? Maybe holes for
locking screws are threaded?
TD> nail driven very distal in the femur looks extremely good.
Without a comparative series we are left to base decisions on
In our settings same nails are used for ante- and retrograde
insertion.
For distal cases presuming particular design of the nail i prefer
antegrade. Retrograde is reserved for unilateral femur+tibia
fractures, problems in the hip region (implants, excessive scars, neck
fractures).
Best regards,
Alexander N. Chelnokov
Date: Sun, 4 Jan 2004 09:06:05 -0500
From: M. Becerra
Dear Alex,
You have shown a very nice case but could you pls answer the
following questions?
1. How was the overall X-ray exposure as compared to that of a
retrograde nail?
thanks and regards
Manuel Becerra MD
Date: Sun, 4 Jan 2004 19:45:11 +0500 From: Alexander Chelnokov Hello M., MB> 1. How was the overall X-ray exposure as compared to that of
a retrograde nail? Never performed retrograde nailing for such a distal fracture so have
nothing to compare with. MB> 2. How did you reduce the distal fragment: open, mini-open,
closed, joystick technique? Closed, by a small wire external distractor. MB> 3. How can you make sure there is no or a slight distal protrusion:
only C-arm, C-arm and X-ray, mini-open? C-arm only, and post-op X-rays, of course. Though as i mentioned before
there were cases of the slight distal protrusion which didn't cause any
troubles. MB> 4. If there is a protrusion how can you make certain there
is no damage to cartilage, PCL? One can be definitely certain about damage of the cartilage only with
direct vizualization (arthroscopic?) - in the case i certain only that the
canal was prepared by awl and the nail was not pulled out to the position.
PCL
must be posterior to the nail - never thought about it. MB> 5. There is an "exact" entry point for the retrograde
nail, how can you control the "exit point"? (Blumensaat's line?) Also with the intercondylar notch at some AP shots with different cranial
deviation.
Best regards,
Alexander N. Chelnokov
Date: Sun, 4 Jan 2004 11:29:11 -0500
From: James Carr
A good summary by Tom. Technically, the retrograde is much easier, and allows
for exact reduction of the condyles by visualization. It also obtains fixation
through the entry tunnel if the nail engages it. I have experienced cases of
arthrofibrosis, and patellar ligament scarring though, so it is a trade off to be
sure. Interestingly, as Alex points out, antegrade nails often have screw holes
closer to the end of the nail.
Jim Carr
Date: Sun, 4 Jan 2004 13:00:32 EST
From: Tadabq
Alex
All good and cogent arguments for antegrade nailing.
Regarding knee motion:
Regarding distal fixation:
But that is theory and you can achieve many of the desired effects with
antegrade technique by driving the nail very distally as in the case shown and
using a nail with very distal locking screws, as you mentioned and illustrated.
That's what makes this case an interesting discussion.
TD
Date: Mon, 5 Jan 2004 22:22:48 +0500 From: Alexander Chelnokov Hello James, JC> easier, and allows for exact reduction of the condyles by visualization. Do you mean arthroscopic control or incision for the nail is large enough
to view/control the condyles? Can you pls describe the technique? JC> It also obtains fixation through the entry tunnel if the
nail engages it. Didn't get the idea - could you pls explain? JC> antegrade nails often have screw holes closer to the end of
the nail. So maybe it takes some re-design of the end of the nail to adopt features
of distal/retrograde nails? BTW can somebody point a source where definitions can be found what first,
second etc generations nails are. THX in advance.
Best regards,
Alexander N. Chelnokov
Date: Mon, 5 Jan 2004 14:05:34 -0500 From: James Carr Alex thanks for the reply- Since the retrograde nail can be placed by
arthrotomy, direct visualization of the fracture is made. No arthroscope
is needed. Secondly, the retrograde nail is placed through a drill hole
in the notch- an area that has good subchondral bone. This creates a snug
fitting tunnel in which the end of the nail can be left, thus providing
some fixation. Hope that helps. I am not aware of a source to define the
various generations of nails.
Jim James B. Carr, MD
Date: Mon, 5 Jan 2004 23:16:24 +0500 From: Alexander Chelnokov Hello Tom, TAC> does come back after a few months just like or better than
other knee operations (e.g., ACL reconstruction). It would be interesting to compare long-term follow up of both techniques. TAC> Hip motion (that you didn't mention) returns to normal faster
and more completely with retrograde nailing than antegrade. Really i didn't check limits of abduction/rotation. But it seems that
functionally significant range of hip motions is not strongly affected. TAC> Hence the concept of "entry site problems are probably
equivalent." Yes, i agree in general - cases of abductor weakness show that there
is no ideal here. TAC> fixation because it is typically placed under direct control Pls add some more details about the direct control. TAC> screws (3 or more) can be placed obliquely in several planes
with nail mounted Not available here yet. Though tibial nails can be used as retrograde
femoral - it has 45 degrees holes except trasverse. TAC> better than the co-linear screws, (which were designed for
and work great for rotation and length control of mid-diaphyseal fractures). Why the holes are not threaded? It would provide greatest angular stability. TAC> using a nail with very distal locking screws, as you mentioned
and illustrated. That's what makes this case an interesting discussion. THX for your as usual very interesting comments.
Best regards,
Alexander N. Chelnokov
Date: Tue, 6 Jan 2004 00:34:09 EST From: Tadabq Alex, 1. Knee motion after antegrade and retrograde nailing of femur
shaft fractures has been reviewed and generally suggests knee motion is
slower to return after retrograde nailing but at 3 months motion is generally
full and equal with the 2 techniques. 2. For distal femur fractures the typical comparison has been between
retrograde nails and plates and the motion is similar with the two techniques,
although some loss of motion is typical. 3. I agree with Dr. Carr's description of the subchondral purchase
of retrograde nails. 4. Threaded distal locking holes in retrograde nails seems
like a good idea but is not yet available, to my knowledge. Locking
plates are gaining great popularity over the past year and do provide for
a construct with outstanding stability. 5. Direct control to me means the relative small distal fragment
can be moved with the partially inserted nail used as a joystick in contrast
to the "indirect" reduction achievable by trying to align the
distal fracture with an antegrade nail. Other percutaneous manipulation/reduction
maneuvers are occasionally required. Rarely would extending the incision
to visualize the fracture surfaces of an extra-articular distal femur
fracture be required. 6. "Generations" are used colloquially in many medical
musings. I would say first generation nails were Kuntscher type
without locking. Second generation were lockable nails. A variety
of products have referred to themselves as third generation (titanium,
sleeved systems, retrograde, active compression nails and the like) but
none have really been a quantam improvement and I doubt there is any consensus
on what, if anything, constitutes a third generation nail as of 2004. TD
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
2. How did you reduce the distal fragment: open, mini-open, closed,
joystick technique?
3. How can you make sure there is no or a slight distal protrusion:
only C-arm, C-arm and X-ray, mini-open?
4. If there is a protrusion how can you make certain there is no damage
to cartilage, PCL?
5. There is an "exact" entry point for the retrograde nail, how can you
control the "exit point"? (Blumensaat's line?)
Lima - Peru
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Knee motion is slower to return after retrograde nailing as you mention, but
does come back after a few months just like or better than other knee
operations (e.g., ACL reconstruction). Hip motion (that you didn't mention) returns
to normal faster and more completely with retrograde nailing than antegrade.
Hence the concept of "entry site problems are probably equivalent."
I think the retrograde nail has better distal
fixation because it is typically placed under direct control more distally in the
distal fragment with potential for nail in the subchondral bone. The distal
screws (3 or more) can be placed obliquely in several planes with nail mounted
guides giving better purchase on the distal fragment than the typical
co-linear transverse screws (often 2 or maybe 3). The clustered oblique screws seem
better at resisting toggling of the voluminous distal fragment around the nail
better than the co-linear screws, (which were designed for and work great for
rotation and length control of mid-diaphyseal fractures).
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Palmetto Health Orthopedics
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia