
Date: Wed, 14 Jan 2004 15:43:50 +0500
From: Alexander Chelnokov
Subject: Subtrochanteric Femur Fx - Peri-Implant
Hello All,
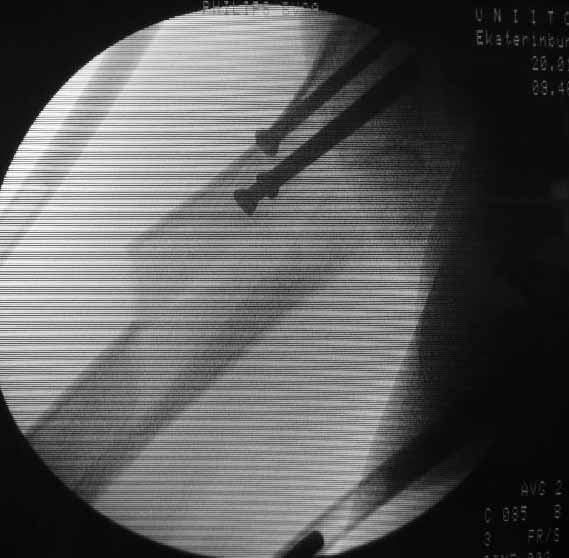
A female 69 years old sustained a femoral neck fracture 2 years ago, which was fixed by lag screws. She has been walking with full WB at home and with cane outside. Today she was trying to sit and missed the chair. X-ray attached. Opinions?
|
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 14 Jan 2004 06:44:48 -0800
From: Chip Routt A lateral film would help.
M.L. Chip Routt, Jr.,M.D.
Date: Thu, 15 Jan 2004 15:19:47 +0500
From: Alexander Chelnokov
Hello Chip,
CR> A lateral film would help.
See attachment for the only one available at the moment.
Best regards,
Alexander N. Chelnokov
Date: Thu, 15 Jan 2004 02:07:20 EST
From: Aobonedoc
Perhaps several cerclage wires, then screw removal and IM nail with proximal
fixation into head. Cerlage wires by themselves are tempting but I suspect
significant risk of failure.
Sincerely and respectively,
M. Bryan Neal, MD
Date: Thu, 15 Jan 2004 08:01:21 -0600
From: Steven Rabin
i'd suggest removal of screws, and fixation with DHS or similar implant
Date: Thu, 15 Jan 2004 08:50:38 EST From: Bill Burman See another case
of a subtrochanteric fracture through screw holes for femoral neck fracture
fixation. Bill Burman, MD Date: Thu, 15 Jan 2004 15:38:55 EST
From: Tadabq
That's a great case illustration provided by Bill and HWBF and the blade
plate/valgus producingosteotomylooks like a good option for Alex's case. A
particularly interesting aspect of Alex's case is the 2 years since screw
placement. We've been leaving proximal screws in place indefinitely for years
and haven't seen very many late fractures around them. The problems, if they
occur, tend to be loss of fixation or early fracture from distal or large or many
drill holes or the occasional arthritic hip requiring screw removal for femoral
prosthetic placement. Perhaps this fracture at two years post opis merely a
very uncommon and unlucky patient? Or have others seen this specific problem
more frequently?
TD
Date: Fri, 16 Jan 2004 12:40:28 +0500
From: Alexander Chelnokov
Hello Tom,
TAC> That's a great case illustration provided by Bill and HWBF and the blade
plate/valgus producing osteotomy looks like a good option for Alex's case.
I am not sure. Is it even technically doable in this fracture
with splitting in frontal plane.
I wonder why so few colleagues supported option of IM nailing.
TAC> femoral prosthetic placement. Perhaps this fracture at two years post op is
merely a very uncommon and unlucky patient? Or have others seen this specific
problem more frequently?
In our settings it is uncommon injury.
Best regards,
Alexander N. Chelnokov
Date: Fri, 16 Jan 2004 12:24:44 EST
From: Tadabq
Regarding this specific patient, it is quite difficult for me to discern the
exactfracture pattern and therefore treatment suggestions. It appears to be a
spiral fracture starting just proximal to the less trochanter and extending
distally 6 or more cm into the shaft with medial displacement of the distal
fragment. The lesser troch is a seperate fragment. The 2 year old femoral neck
fracture appears to have healed in good position I really can't tell where the
fracture starts laterally, but presumably it's near the distal most screw. I
can't tell if there is further comminution of the shaft or the greater
trochanter.I can barely see the fracture on the lateral radiograph. I'm not
sure but I don't see AVN of the femoral head nor OA of the hip. Her overall bone
quality appears normal for a 68 year old. I don't see any loosening of the
screws but I can't tell for sure. The fracture extention well into the shaft
makes intramedullary fixation somewhat more appealing than plate fixation and
contrasts with the case posted by Bill. A reconstruction nail with proximal
locking into the femoral head and neck after screw removal and reduction would be
reasonable.
TD
Date: Fri, 16 Jan 2004 16:50:05 EST From: Bill Burman As has been suggested, better xrays are required to rule out femoral
neck non-union, femoral head AVN, subtrochanteric fx extension to the piriformis
fossa, etc. In the absence of all of the above, per Tom DeCoster's description,
the subtrochanteric fx appears to be a Russell-Taylor Type 1B which, in Toney Russell's OTA
Basic Fx Course Lecture, is recommended for fixation with a cephalomedullary reconstruction IM nail. In the same talk, blade-plating with indirect reduction technique receives honorable mention.
Bill Burman, MD Date: Tue, 20 Jan 2004 12:48:52 +0500
From: Alexander Chelnokov
Another lateral view.
A closed nailing is scheduled for today. No
reconstruction nail is available so a usual one is planned.
Best regards,
Alexander N. Chelnokov
Date: Tue, 20 Jan 2004 21:48:57 +0500
From: Alexander Chelnokov
Hello All,
TAC>A reconstruction nail with proximal locking into the femoral head and
neck after screw removal and reduction would be reasonable.
The screws were removed through a stab wound. Then a closed insertion
of an unreamed solid nail 13 mm was performed and the nail statically
locked - 3 screws 6 mm in the proximal fragment and 1 in the distal.
Considering varus of the healed neck i tried to get some valgus to the
proximal fragment as the nail allowed. The result attached. The
fracture pattern can be seen better than in the initial films.
Best regards,
Alexander N. Chelnokov
Professor-Orthopedic Surgery
Harborview Medical Center
325 Ninth Avenue
Seattle, WA 98104-2499

Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005
HWB Foundation
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
HWB Foundation
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Any comments?

Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia