
Date: Tue, 21 Dec 2004 18:27:03 +0500
From: Alexander Chelnokov
Subject: Pelvis malnonunion
Hello All,
Dear colleagues
A female 27 years old admitted to our unit. Injured 18 month ago in a car accident. Initially the pelvis was fixed by anterior frame. 1 month later hardware was removed because of pin tract infection, and walk with cruches allowed. Also reptroperitoneal haematoma got infected.
She was referred to our unit 3 month ago. There was a perineal sinus, so she was sent back to her local surgical hospital, where the sinus was debrided, and about 1 liter of pus removed from the femur. The sinus closed 6 weeks ago. She walked with crutches.
Now there is shortening ~5 cm, no walking aids, of course obvious limp. No signs of infection neither clinically nor in lab tests. Which is optimal management for now? Only to move down the acetabulum (by which approach?), or full reduction of anterior and posterior aspects, acutely or gradually?
|
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 22 Dec 2004 08:09:45 -0800
From: Chip Routt
Hi Alex-
It 's too bad to miss caring for her acutely.
The infection history and recurrence complicate the situation, and you will need to sort that out clinically and radiographically as necessary.
Should you deem her fit for surgery, the 3-D CT alone is insufficient for planning preoperatively. We can t see the healing response, soft tissue envelope, the right SI injury, nor the left SI joint problem well enough on the 3-D CT alone.
Based on what you ve shown-
1. Ignore the left sided SI joint malunion, assuming that it is stable...is that accurate? If not, start there with a debridement, reduction, and fixation of your preference.
2. Then plan for a long OR day and use a blood salvage suction system.
3. First approach the greater sciatic notch limb of the injury using a KL exposure, debride that portion of the fracture, and also sharply release the contracted local soft tissues such as the sacrospinous and sacrotuberous ligament complexes...then close and turn supine.
4. Use an ilioinguinal exposure to release all local soft tissue tethers, debride the iliac limb, the ipsilateral ramus, and the contralateral ramus injuries. You can also debride and mobilize the right sided SI joint if it s indicated.
5. Then start moving the right floating acetabular segment back home. This may require clamps or other manipulation techniques. Sometimes the distractor can be used if the contralateral posterior pelvic ring is stable (which takes us back to the #1 comment above). Some like a traction table or other manipulating reduction techniques.
6. Fix the all fractures and their limbs with stable fixation of your choice. Lag screws, buttressing plates, and other smart fixation would be good for her.
7. Some might prefer a period of postoperative traction, or other creative external skeletal support....you ve demonstrated skill with such devices in the past!
8. Have an ICU bed ready for her after surgery
Or you can just strategically insert some wires where they need to be, hook up some rings and threaded bars creatively, move it all around magically, and show us the perfect result without scars nor infection....at least that s been your history, so I remain suspicious!!
That s about it-
Chip
Date: Sat, 25 Dec 2004 00:03:28 +0500
From: Alexander Chelnokov
Hello Chip,
THX for the valuable reply.
CR> 1. Ignore the left sided SI joint malunion, assuming that it is stable...is that accurate? If not, start there with a debridement, reduction, and
Interestingly, the left sideâ SI joinnt is the only painful focus for now.
CR> 2. Then plan for a long OR day and use a blood salvage suction system.
We here will think on it next weeks, i suppose the surgery is to be scheduled not earlier then Jan 10-12 in the next year...
CR> Or you can just strategically insert some wires where they need to be, hook up some rings and threaded bars creatively, move it all around magically
THX for the brilliant idea! :-)
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 22 Dec 2004 9:43 PM EST
From: Bill Burman
Chip
>3-D CT alone is insufficient for planning preoperatively. We can't see the healing response, soft tissue envelope, the right SI injury, nor the left SI joint problem well enough on the 3-D CT alone.
How useful for preop planning are actual 3D models produced by stereolithography or other rapid prototyping techniques reported by Brown et al - OTA 2002.
Date: Fri, 24 Dec 2004 00:55:00 EST
From: Tadabq
A 3 dimensional life size model of this pelvic malunion could be easily made from the CT scan with minimal cost and would provide the surgeon the ability to see the bone and deformity without soft tissues. That would seem to facilitate freeing up the partially healed fractures and reducing them.
TD
Date: Tue, 28 Dec 2004 19:00:48 +0500
From: Alexander Chelnokov
Dear colleagues,
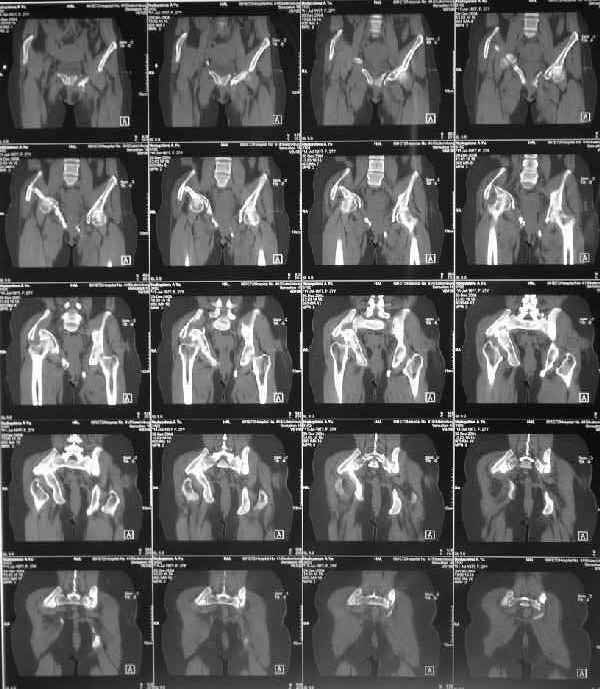
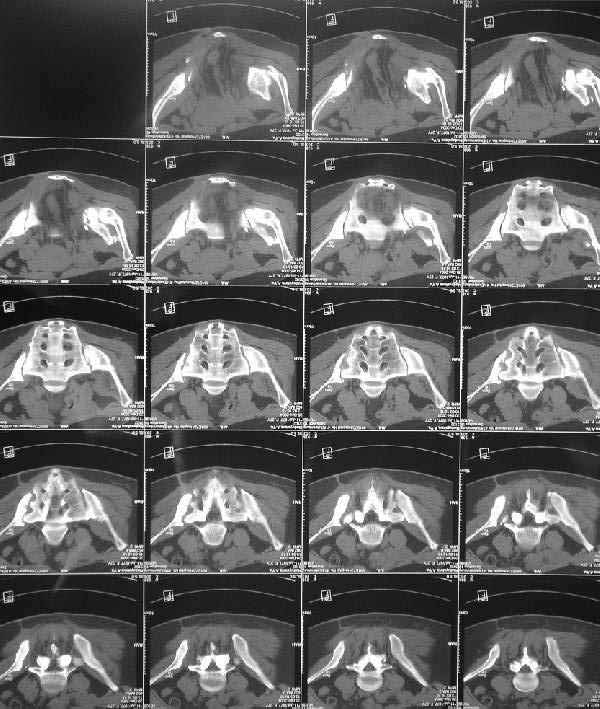
Some additional data. Her main complaints are:
-pain in the left SI joint, the right is painless;
-limb shortening (walks with shoe raise, no walking aid)
-scoliosis and extra-lordosis
-low back pain
-unable to stand more than 20-30 minutes
-unable to sleep without inflatable rubber pad under the sacrum and bolsters under knees.
-unable to sit comfortably
Majeed score is 41.
X-rays and more CT - see attached.
 |
 |
 |
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 7 Mar 2005 00:34:26 +0500
To: OTA LIST From: Alexander Chelnokov
Dear colleagues,
RE: The case of pelvic malunion discussed 8 weeks ago.
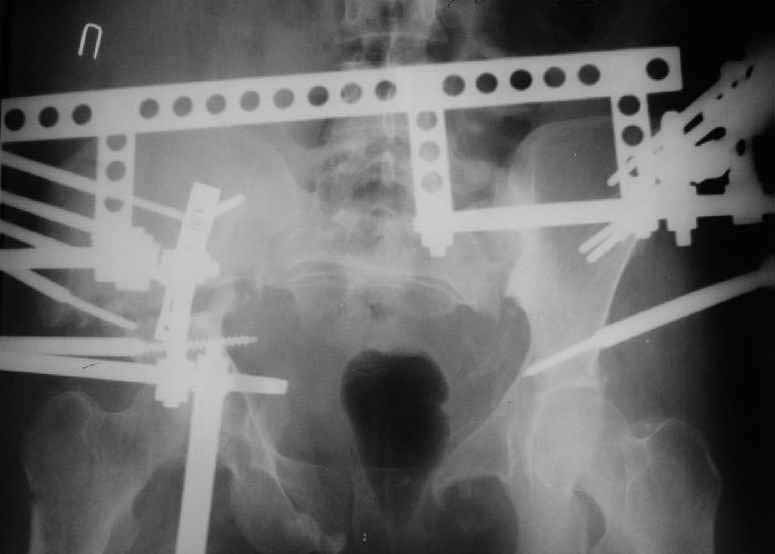
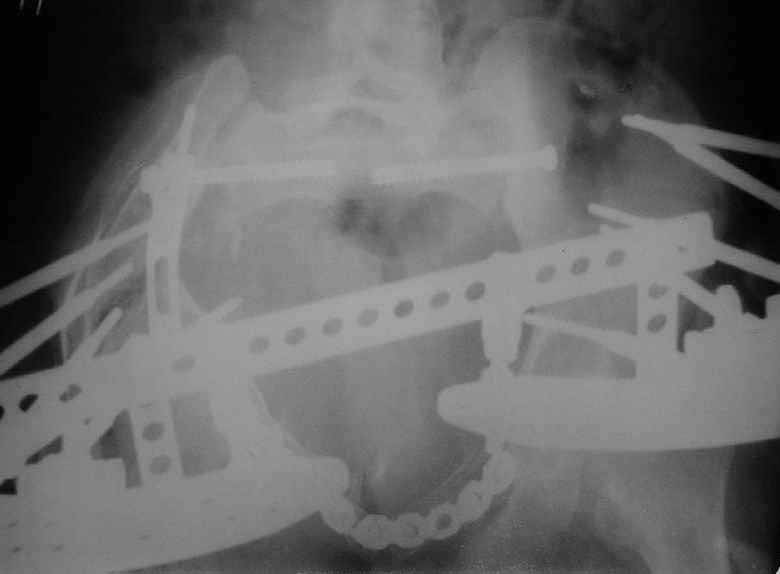
On Jan 26, 2005 the right wing was osteotomized, its segment with the
acetabulum was moved downwards, the ilium was plated, and pelvic external
fixator with femoral extension applied (left image).
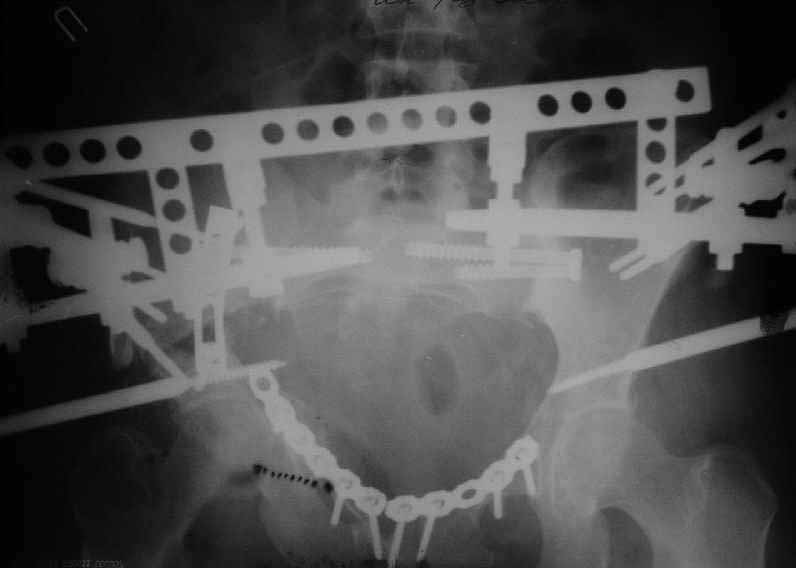
After wound healing, anterior reconstruction was performed, iliosacral
screws inserted, the femoral frame removed.
To date wounds healed, the patient walks with crutches, no
weight-bearing at the right side (rest images).
Expecting your comments/opinions, THX in advance.
Best regards,
Alexander N. Chelnokov
Date: Sun, 06 Mar 2005 20:41:28 -0800
From: Chip Routt
I hope that she'll be better...it's hard to see much on the images with the frame structure on it.
Chip

Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
{kind=link}