
Date: Date: Fri, 12 Aug 2005 22:35:49 +0600
From: Alexander Chelnokov
Subject: Forearm fracture
Hello All,
A male 51 years old admitted to our unit 4 days after industrial trauma (a heavy piece of metal fell on the forearm) already in a plaster cast. Swelling was so significant that compartment syndrome was expected but he still has been demonstrating good sensation and movement of fingers. Also there were 2 sites of skin necrosis 3x1 cm, with serous drainage. He was left in the plaster for a week - looks better now. Swelling decreased, no pus. What surgical option should be preferred? As i realize, primary alternatives are closed nailing and external fixation? THX in advance.
|
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sat, 13 Aug 2005 19:33:31 -0700
From: John Ruth
Current standard in US is ORIF with compression plate and screws.
Date: Sun, 14 Aug 2005 15:39:48 +0600
From: Alexander Chelnokov
Hello John,
JR> Current standard in US is ORIF with compression plate and screws
Don't you expect the current state to be changed? What advantage do we have with ORIF and plates comparatively for example to Smith & Nephew's Foresight locked nails inserted without fx site opening?
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sun, 14 Aug 2005 09:40:49 -0700
From: John Ruth
We have a history with plates and they work in the forearm. Do rods work as well? Just because they are less invasive doesn't necessarily make them better. Are you familiar with a prospective study doing a head to head comparison of compression plates vs. locked IM rods in the forearm?
Date: Mon, 15 Aug 2005 01:53:00 +0600
From: Alexander Chelnokov
Hello John,
JR> We have a history with plates and they work in the forearm. Do rods work as well? Just because they are less invasive doesn't necessarily make them better.
Why? Some benefits of less invasive technique are self-evident.
JR> Are you familiar with a prospective study doing a head to head
It is obvious that closed nailing is very promising technique for the forearm so IMHO at this period studies are necessary how to refine and standardize technique of forearm nailing. Otherwise good plating would be compared with bad nailing.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 16 Aug 2005 01:34:44 +0600
From: Alexander Chelnokov
Hello All,
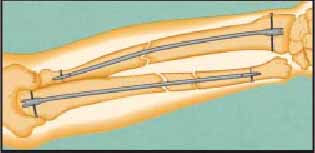
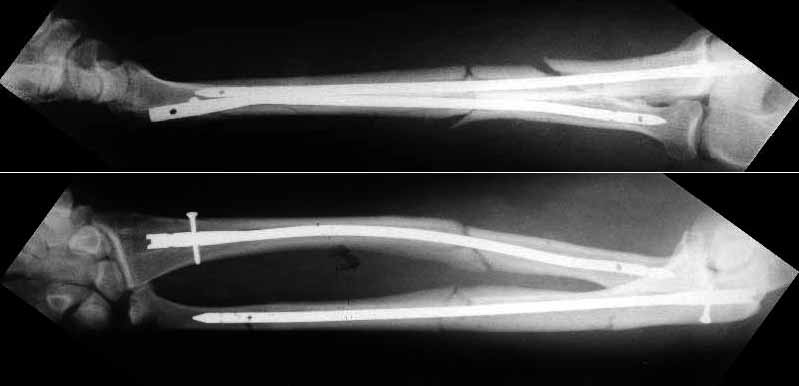
Closed nailing was performed by 4 mm stainless steel implants (ChM, Poland). I decided to lock both dynamically because of shape of bone ends which prevents rotation and telescoping. Images attached. Comments and critics are welcome.
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
From: Jeff Brooks
Date: Mon, 15 Aug 2005 16:41:30 -0400
Are you going to immobilize him in a long arm cast or let him start motion?
The reductions are nice, but I'd be concerned that the fracture of the radius will move with pronation & supination encouraging nonunion (since the nail is essentially fixed to the distal radial shaft and free to move with respect to the proximal radius.
I'd lean toward 4-5 weeks in a long arm cast, giving him "credit" for the past week or so of immobilization.
Overall, very nice.
Jeff Brooks
Stamford, CT
From: Alexander Chelnokov
Date: Tuesday, August 16, 2005, 1:15:50 PM
Hello Jeff,
JB> Are you going to immobilize him in a long arm cast or let him start motion?
No, only a sling.
JB> The reductions are nice, but I'd be concerned that the fracture of the radius will move with pronation & supination encouraging nonunion
I suppose it won't because of shape of bone ends and also 3 point fixation by the bent nail.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 15 Aug 2005 16:30:24 -0700
From: John Ruth
The reduction is excellent but I am not sure that you have rotational stability of the proximal radial fragment (no proximal locking) this could rotate with pronation and supination. If you are planning to cast then ORIF with plates is superior because casting is not necessary. I would expect these fractures to heal with callus as opposed to primary bone healing seen with plated fixation. Is healing with callus in the forearm a problem? I am not sure I know. How do these rods and locking screws compare price wise with plate and screw fixation (more expensive I would expect)? How often is hardware removal required? What was your operative time? I think these are all factors to consider when comparing a new treatment method with an established one.
From: Alexander Chelnokov
Date: Tuesday, August 16, 2005, 1:53:48 PM
Hello John,
JR> stability of the proximal radial fragment (no proximal locking) this could rotate with pronation and supination.
I tried rotation under image inensifier and all looks stable enough. Of course he won't be encouraged to perform forced rotation immediately.
JR> If you are planning to cast
No.
JR> would expect these fractures to heal with callus as opposed to primary bone healing seen with plated fixation. Is healing with callus in the forearm a problem? I am not sure I know.
It is not a problem. We have some experience with rectangular-pentagonal titanium nails without screws - early functional recovery is a common result.
JR> How do these rods and locking screws compare price wise with plate and screw fixation (more expensive I would expect)?
You are right especially if compare domestic plates with rods from abroad. The rod here is ~$300. But i suppose with time prices will be balanced at reasonable level depending on how many implants are sold.
JR> How often is hardware removal required?
I hope not to touch asymptomatic implants.
JR> What was your operative time?
A bit less than 2 hours. But since it was only my second surgery with implants of this type and i still was discovering its features, the time must be shorter with more experience.
JR> I think these are all factors to consider when comparing a new treatment method with an established one.
Of course. But i suppose we have at first to sqeeze it to its utmost and then compare.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 15 Aug 2005 21:01:09 -0400
From: Brent Bamberger
Excellent
Actually plating would have been very difficult and would have added possible complications. Long arm cast for 2 weeks then Active ROM would be my approach. Is the elbow OK ?? radial head looks a little posterior though???
H Brent Bamberger DO
DME Grandview Hospital
Program Director Orthopedic Surgery
From: Alexander Chelnokov
Date: Tuesday, August 16, 2005, 3:03:52 PM
Hello Brent,
BB> Actually plating would have been very difficult and would have added possible comlications.
OMHO quite reasonable.
BB> Long arm cast for 2 weeks then Active ROM would be my approach.
Never used cast after nailing of the forearm shaft.
BB> Is the elbow OK ?? radial head looks a little posterior though???
The elbow presented no pain. Motions were free at the table. Will check later.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 17 Aug 2005 08:31:43 -0400
From: Jeff Brooks
Very nice case. Thanks for sharing it.
Jeff Brooks
Date: Thu, 10 Nov 2005 20:03:29 +0500
From: alex
Dear Jeff and colleagues,
JB> Please make a note of letting us know how this patient is doing
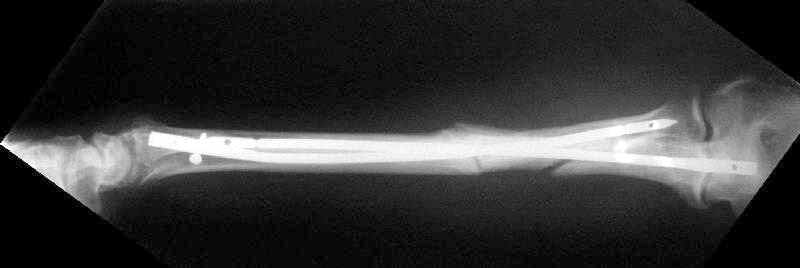
He just visited the clinic in 3 months after the surgery. X-rays
attached. He ignored any physio and ROM excersices so his
functional status is not the best i ever seen.
Best regards,
Alexander N. Chelnokov
Stamford, CT





Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia