

Date: Sat, 15 Oct 2005 00:35:12 +0600
From: Alexander Chelnokov
Subject: Neglected femoral neck fx
Dear colleagues,
A male 31 years old treated elsewhere after not severe pelvic fracture 2 months ago, was managed non operatively. So the injury looked as a reason of his inability to elevate the leg. However at the recent x-rays the neck fractire was found. The patient already has been walking with partial weight-bearing.
Looking at the x-rays and the time since the injury, what is the optimal treatment for now? We discussed 1)leave as is, 2)2 cancellows screws as is, 3)valgus osteotomy. Total hip replacement looks unnecessary yet.
What is your opinion? Which option from the listed or something else should be preferred and why?
|
|
THX in advance.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str. Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sat, 15 Oct 2005 10:44:22 +0300
From: Erden Kilic
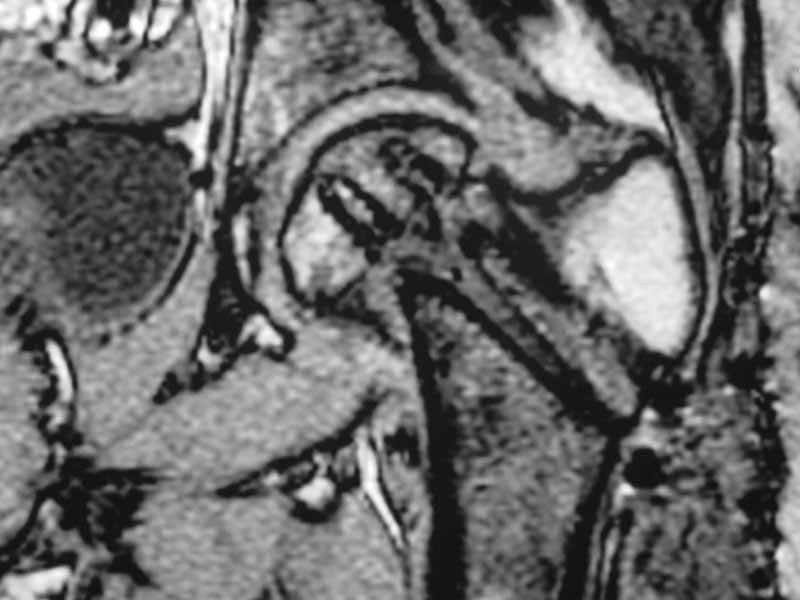
I would leave it as it is. Because surgical intervention will not be able to prevent osteonecrosis if it is going to be. MRI may be helpful to determine union if there is any and also gives an idea about the viability of the head.
Erden Kilic, MD
Gulhane Military Medical Academy
Ankara, Turkey
Date: Sun, 16 Oct 2005 13:31:50 +0800
From: Sam
Dear friend:
If I were u , a DHS will be used to fix it . And I will tell the patient not to weight bearing from now on. It will accelerate the aseptic necrosis of the femoral head.
Best wish to U
Dr. Sam. Shen
Dept. of Othropaedic and Trauma
Xin-hua hospital
Shanghai, P.R. China
Date: Sun, 16 Oct 2005 21:42:17 -0400
From: saklmmq
friend
dhs will not correct improper improper biomechanical environment� and may further compromise vascular integrity
consider:
establish vascular status via mri and if viable follow with proximal valgus osteotomy�
case provided s/p failed fixation
 |
 |
 |
stephen kottmeier
Date: Sun, 16 Oct 2005 23:10:57 -0400
From: Peter Trafton
I think that this 31 yo deserves a try with valgus osteotomy, as so nicely illustrated by stephen kottmeier. However, I'd do it no matter what an MRI shows - thus why bother with the MRI? (What sort of data support MRI's ability to predict segmental collapse?)
�/pgt