
Date: Tue, 22 Feb 2000 21:09:22 -0500
Subject: Bladder Herniation - Pelvic Malunion
From: Fred Barrick
OK, Here's another case.
A 41 year old woman is referred by a reconstructive gynecological surgeon because of a urinary bladder herniation through a disrupted anterior pelvic ring.
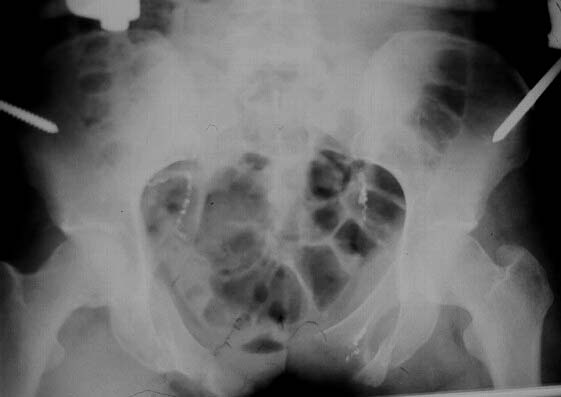
The patient sustained multiple injuries 11 months previously, including the pelvic ring disruption seen in the attached photos. The anterior injury was a fracture through the left pubis; the posterior lesion was a vertical fracture of the sacrum.
|
Initially an exfix was used at a university hospital trauma center.
 |
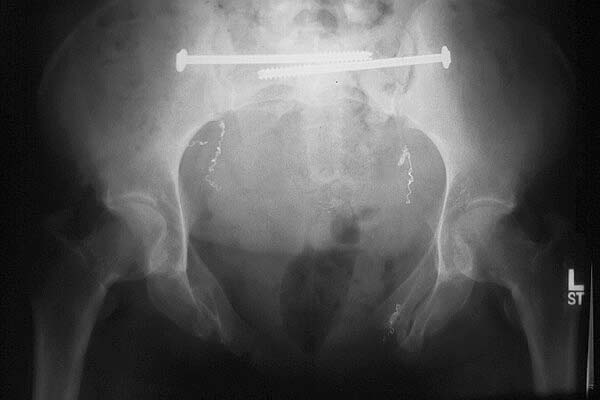
Four months later bilateral iliosacral screws were used for an apparent nonunion of the sacral fracture.
 |
An exfix was reapplied two months thereafter, apparently to try to reduce the now widened anterior pelvic ring defect. It was removed after a short period of time, probably because it was ineffective. The orthopaedic surgeon told her that he would not fix the anterior pelvis under any circumstances.
She now presents with a large bladder herniation (sorry, I have to reshoot the photo of the dramatic CT).
 |
 |
 |
She has considerable pain in the pubic region and some pain posteriorly. She has burning pain in the left anterior lateral left thigh in the distribution of the anterolateral femoral cutaneous nerve---secondary to one of the exfix pin insertions. The anterior gap measures about 8 cm. Anterior fixation and bone grafting is planned. The question is: Can this big a gap be closed with just an anterior approach?
E. Frederick Barrick, MD, Director of Orthopaedic Trauma, Inova Fairfax
Hospital, Falls Church, VA
Date: Wed, 23 Feb 2000 09:32:21 -0500
From: Mark C. Reilly, M.D.
In analyzing this case, I would look at three issues, the deformity of the posterior pelvic ring, the anterior pelvic ring and the urologic dysfunction.
The Xrays and CT's provided show evidence of a Right sacral ala fracture, healed without significant vertical displacement or rotational abnormality. There is no evidence of external rotation through either of the SI joints. I see no evidence of there being a nonunion of a sacral fracture. I am unclear about the original purpose of the iliosacral fixation. Perhaps pre-op Xrays prior to this procedure would be helpful. In any event, there does not appear to be a substantial posterior pelvic ring deformity at this time. This is supported by the current AP pelvis which demonstrates well defined ilioischial lines bilaterally with a well positioned AP of the sacrum.
The anterior pelvic ring injury probably consisted of Bilateral superior and inferior ramus fractures as well as a fracture of the body of the pubis. The rami have united with the large anterior diastasis. I believe, therefore, that this is an isolated malunion of the anterior pelvic ring ocurring through 3 sites, the rami bilaterally and the body of the L pubis.
The reconstruction of this deformity may be corrected with bilateral superior and inferior ramus osteotomies and an open reduction of the body of the pubis all performed though a Pfannenstiel approach. Internal fixation could either be performed with a single long plate spanning both rami osteotomies and the symphysis or with 2 plates. The plate stabilizing the pubis body fracture would have to cross the symphysis to achieve appropriate fixation. Given that a urologic reconstruction is planned, the rami osteotomies and the pubis fracture need to be quite stable as there will be a substantial amount of soft tissue stripping for the bladder mobilization. In most cases, though, you can avoid circumferential soft tissue stripping around the rami osteotomies and reduce the anterior ring by "hinging" these closed. Since the purpose of the urologic reconstruction will be to get the bladder scarred down solidly to your reconstruction so the last thing you want is to have to contemplate going back in for a non-union so I would probably bone graft all sites at the time of the initial reconstruction.
Occasionally, due to bone loss or shortening at the displacement sites, the anterior ring is unable to be closed without creating distraction of the rami osteotomies. Making these osteotomies obliquely allows some additional length while still maintaining bony contact. In my experience with anterior malunions and my time spent with Joel Matta this has been a successful means of treating this difficult problem. Rarely, a closing wedge osteotomy of the anterior sacral ala is necessary to get the anterior ring closed but I don't think it will be necessary in this case. If it is, it can be performed by extending the Pfannensteil into an ilioinguinal for access to the SI joint and anterior sacrum.
I enclosed a similar injury Xray. Although this patient has anterior SI widening on the left, he has the same anterior ring injury. B rami and a fx-dislocation of the symphysis.
 |
Mark C. Reilly, MD, Co-chief Orthopaedic Trauma Service, New Jersey Medical School
Date: Thu, 24 Feb 2000 10:13:42 -0600
From: Adam Starr
I'm suspicious that she may have been fixed in a malreduced position in the back. Do you have inlet and outlet views that show the posterior reduction is good?
If things are fine posteriorly, then I would think that you could correct the anterior deformity with an anterior operation. Bilateral ramus osteotomies should work, both superior and inferior, followed by plating of the symphysis.
Good luck.
Adam Starr
Date: Thu, 24 Feb 2000 10:19:43 -0600
From: Adam Starr
Another way to fix the injury Dr. Reilly showed would be to stabilize the rami fractures with screws instead of plates. You could reduce both ramus fractures and stabilize them with cannulated screws (can be placed either antegrade or retrograde) and then plate the symphysis.
Once the symphsis and anterior ring are fixed, you could assess the posterior ring and see if it needed to be stabilized, too. In this view it looks like it might not need anything once the symphysis is done.
The nice thing about the ramus screws is that you don't have to do as much soft tissue dissection as you would with a plate. You'll have to do something close to a complete ilioinguinal approach to plate that high ramus fracture on the patient's right. The plates should work fine, but if I was that patient, I would rather have a ramus screw and the lesser dissection than a big ORIF with a plate.
Just my 2 cents.
Adam Starr, Dallas
Date: Thu, 24 Feb 2000 11:50:27 +0100
From: bruce meinhard
I would agree with Mark that the bone problem is the lesser of her difficulties. The posterior pelvis looks like it was adequately and anatomically repaired. The anterior pelivis could be better approximated by a sliding oblique osteotomy in the coronal plane of the anterior structures of the pelvis through an anterior approach( Pfannensteil with extension to ilioinguinal if needed). Plate fixation as well as bone grafting are also of value.
The Uro-Gynecologist may also have to perform a ligamentous reconstruction with GorTex or freeze dried fascia. I have participated in one patient who had such reconstruction and she resorbed the allograft. She had an intense inflammatory reaction that lasted acutely for several weeks. This presented as a rule out possible infection. Subsequently all failed except the bone work and revision surgery succeeded with the use of GoreTex.
BPM
Date: Thu, 24 Feb 2000 15:45
From: Bill Burman
Questions to the pelvic gurus:
1) Seems like there is some disagreement about whether the pelvic deformity is anterior vs posterior.
The posterior pelvic contours look normal on CT but what if (for the sake of argument) the patient had bilateral posterior iliac fxs that malunited symmetrically in external rotation?
At the 1999 OTA Basic Fx Course Kyle Dickson said:
"In a study we (Matta, Dickson et al) presented at the OTA as well as the AAOS, we looked at how well the clamps (anterior ex fix) reduced these injuries (APC2, 3 and VS) . 67% of the patients showed increased deformity posteriorly. "
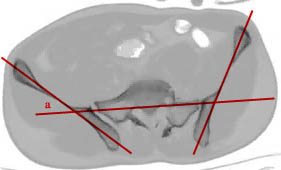
He then showed some representative CT scans with lines drawn on them similar to what is shown below.
 |
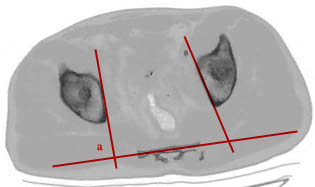 |
I can find no references about this quantitative method (iliosacral or quad_sacral lines or angles) of determining whether or not there is a transverse plane posterior deformity and how big it might be. How exactly are these lines drawn? Are there any normal values for the angles of their intersection?
I have an old graphic of some measurements on an inlet view from Dana Mears but these seem to be relative values and I don't suppose they are used much.
 |
2) When planning a relatively minor rearrangement of a bunch of teeth in an open mouth, our orthodontic brethren go to all sorts of extremes with the creation of models upon which they can scheme a nice smile. Are they so stereotactically bereft or are we so stereotactically gifted that we can afford to forego all that when planning a reconstruction of the pelvis (which seems to contain all the major nerves and bleeders of the body)?
Until recently, decent 3-D modeling of deeply seated anatomic structures has been hard to come by. Relatively recently a process called stereolithography has become available. A laser circles a vat of liquid monomer and according to data provided by a 3-D spiral CT, laser energy is imparted at specific three dimensional coordinates turning liquid monomer into solid polymer. Thereby a solid model is built with reasonably realistic and smooth contours in a process which has been dubbed "printing in 3-D".
I know that Dr. Joldas Kuldjanov at Detroit Receiving (on the left in the picture below) has been working with this and I believe that even Jeff Mast has found a few of his models to be helpful.
 |
What I would do with this case is have several of these models made and then send them to Drs. Mark Reilly, Jeff Mast, Joel Matta, Dana Mears . . . and to whomever returned me the best reconstructed model would I send the patient.
Bill Burman, HWB Foundation
Date: Thu, 24 Feb 2000 20:33:38 -0600
From: Gregory J Schmeling
This is a difficult deformity. The initial anterior ring injury looks sort of lined up on the ex/fix films yet later on there is a large anterior gap. The posterior ring injury looks lined up. That seems incorrect. How could there be such deformity anteriorly and little or none visible posteriorly?
The problem is how to close the ring anteriorly so the GYN's can stuff the bladder, etc., back where they belong. A soft tissue reconstruction, i.e., gortex or allograft has failed in cases I have seen. The GYN'S are more likely to succeed with closure of the anterior pelvic ring. One option to consider is to do bilateral (unilateral???) osteotomies of the iliac wing anterior to the SIJ into the greater notch. Close and plate the anterior ring and then plate both of the osteotomies. I hope she is not obese. Good luck.
Gregory J Schmeling, Chief Orthopaedic Trauma Service, Dept of Orthopaedics, Medical College of Wisconsin
Date: Fri, 25 Feb 2000 11:54:12 -0600
From: Adam Starr
I agree that the anterior deformity in the ex-fix films and the anterior deformity we're shown now appear to be very different.
I wonder how it went from point A to point B?
Still, I think the current deformity IS just an anterior ring problem - the posterior elements that we can see look normal. It would be nice to have inlet and outlet views to be sure.
I agree that a correction of the bony deformity is the best chance of success. Mesh or goretex are not gonna hold the bladder in the face of a huge symphsis diastasis.
Adam Starr, Dallas
Date: Sun, 27 Feb 2000 00:23:58 -0600
From: Steven Rabin
i agree that the deformity all appears to be anterior, but it is probably so contracted that i strongly suspect that posterior osteotomies will be necessary to loosen things up enough to bring the front together.
Of course, i'd want to very carefully check his clinical exam - specifically is he walking with his legs externally rotated or straight ahead or is he intoeing? i would worry that if he is straight, then posterior osteotomies would rotate his legs in and he'd be unhappy with his final gait pattern. If he is externally rotated already then the osteotomies would probably help. If he is walking straight, and to avoid the large operation of posterior osteotomies with associated potential complications, i wonder if some sort of fibular or other strut graft across the front would be adequate to hold the bladder in place. good luck.
Date: Wed, 1 Mar 2000 14:52:57 -0600
From: Kyle Dickson
fred
interesting case which i'm not sure what to do. i have fought with the dilemma of open book pelvis with si joint looking pretty good. an osteotomy posteriorly is possible but a huge case with questionable benefits. i do these for one sided usually vertically displaced. i have two cases where i attempted to squeeze them anteriorly with double platting (gap 3-5 cm) with success so far but i'm still worried about them. if you have any questions let me know. let me know what happens.
kyle dickson
Date: Fri, 3 Mar 2000 10:57
From: Bill Burman
Fred
Just received a call from Djoldas Kuldjanov at Detroit Receiving. As a contribution to the discussion of the case of a pelvic malunion with bladder herniation, he said he would make a 3-D stereolithography model of the patient's pelvis "on the house".
He would need preferably GE CT scanner format of no larger than 2 mm cuts on a 5.25 inch magneto-optical cartridge.
His contact info is:
313-993-8675 DRH Office direct
313-745-3415 DRH Office
734-677-0957 Cyber Orthology
Bill Burman, HWB Foundation