{kind=link}





Sun, 20 Feb 2005 02:17:42 +0500
From: Muhammad Amin Chinoy
Subject: Pipkin IV fracture
Dear all
Kindly opine the following problem:
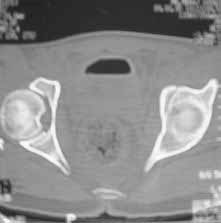
Male 22 yrs of age, RTA, front seat passenger in a truck. Sustained grade IIIB fracture of Tibia, and a Posterior dislocation of the Ipsilateral Left Hip.
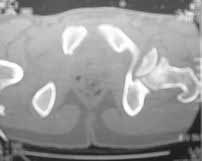
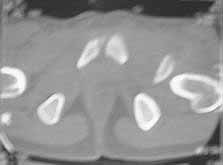
Emergent closed reduction performed, and Tibial wound debrided. Next day Exfix applied and fibula plated. Initially femoral head fracture was not appreciated and it was thought that this is a posterior wall fracture. Presently two weeks down the line, Tibial wound is better but not completely healthy. and plastics want to wait for another five days, before they flap it. I enclose radiographs, Judet view, Ct scans in this and following mails.
Will appreciate your input.
|
|
|
| |
 |

| 
| 
|  |
 |

| 
|  |
Thanks
Dr. M. Amin Chinoy FRCS.
Date: Sat, 19 Feb 2005 15:22:11 -0800
From: Chip Routt
Reduce and fix it as we've outlined on this list several times before...maybe Bill can reference the prior discussions of anterior femoral head displaced fractures.
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
Date: Sat, 19 Feb 2005 20:52:03 -0500
From: Bill Burman
>prior discussions of anterior femoral head displaced fractures.
Bill Burman, MD
HWB Foundation
Date: Sun, 20 Feb 2005 16:51:25 +0500
From: Muhammad Amin Chinoy
Thanks - My queries:
1) Timing. He still has a open tibial wound, and it is more than two weeks. Should it be done later or at the same time as the flap? What are the chances of infection ?
2)The femoral head fracture involves the anter-inferior part and not the weight bearing superior dome. Also while moving the hip after taking weight off the traction, it does seem pretty stable. Should it be fixed even then?
3)You mentioned 2 mm screws. Can a standard 3.5 mm radius ulna screw be used without risk of furhter fragmentation?
4) Would simple excision of the fragment make the head unstable?
Thanks
Muhammad Amin Chinoy
Date: Sun, 20 Feb 2005 08:50:32 -0800
From: Chip Routt
You can do whatever you want to do, and you can rationalize/justify anything that you do.
What would you do to the patient if he was your son? Or you at 22 years old?
Some surgeons believe that a spherically reduced and concentric hip joint is important for durability.
For that reason, those surgeons will work hard to restore hip joint congruity especially in a young adult.
It doesn't mean that they are right.
I can't see his tibial wound and even if I could, I'd debride the tibia and its open wound until it was clean.
Then I'd expose the hip using a modified Smith Petersen exposure. I'd spare the LFCN branches and tenotomize the rectus common tendon.
I'd open the capsule anteriorly using an oblique T-shaped capsulotomy with the vertical limb of the T paralleling the femoral neck and the upper limb of the T paralleling yet sparing the labrum.
I'd remove the displaced and malrotated head fragment, clean it on the back table, apply 2 or 3 glide holes, then clean the hip joint of debris, look at the acetabular fracture thru the joint and assure that it hasn't further displaced.
Then on the clock deliver the shaft/neck/head fragment into the wound (some call this a "surgical dislocation"), then I'd orient/reduce the fragment from the back table onto the "surgically dislocated" fragment, assure that it's reduction was visibly perfect, hold it with K wires inserted thru the fovea central is area to avoid further damage to the head, secure that reduction with small screws using the previously applied glide holes, bury the heads to the subchondral bone level, remove the wires, and place the unit back into the acetabulum.
The "surgical dislocation" usually lasts about 7-10 minutes by the clock depending on the amount of peripheral comminution.
Then do a passive range of motion to assure stability...it will be.
Wash the wound and hip joint. Close the capsulotomy, repair the rectus tenotomy, close the wound, spare the LFCN branches. Then move the hip after surgery.
We recommend some form of HO prohylaxis based on what we've learned.
No one knows the chances of infection.
Based on the selected images that you shared with us, I would not leave it as is. The fragment is significant in terms of its size and location and displacement.
Standard 3.5 mm screws can be used but they have a more prominent head profile than the smaller screws. Further fragmentation due to the screws will depend more on their location and application than size.
In order to accurately reduce this fracture, you'll need to remove it from the hip joint and wound in order to prepare it for fixation. When it is out of the joint, you can perform a passive range of motion to assess the hip joint stability. Typically, hip stability is determined by more factors than simply the size of the fracture fragment alone.
Your concerns are appropriate, but should not paralyse your care.
Treat him like you would want to be treated, and you'll make the correct decisions-
Chip