





Date: Wed, 14 Jun 2000 20:56:22 -0400
Subject: Acetabular Fracture - 91 y o patient
From: H C Cole
Active 91 yo female who tripped on a step and fell while working as a volunteer, sustaining fracture to the right acetabulum. She was community ambulator prior to injury. Minimal medical problems given her age -- Hypertension (well controlled), anemia, mild COPD (chronic obstructed pulmonary disease)with mild hypoxemia, history of intertrochanteric fracture left hip 1998, and inability to tolerate any oral or parenteral narcotics (nausea and vomiting even with Darvocet, even when young.)
|
|
|
|
|
|
The inlet view is perhaps the most impressive. Any insight, thoughts, personal experience(s),and/or views on management in your communities would be helpful.
Thanks,
H C Cole, MD, Steamboat Springs, CO
Date: 14 Jun 00 18:12:58 -0800
From: M.L.Chip Routt,Jr.,M.D.
when was the injury?
a ct would be helpful for accurate planning/decision making.
chip
Date: Thu, 15 Jun 2000 09:28:30 -0500
From: Steven Rabin
she's a "young" 90 year old and wants to maintain an active lifestyle. Her hip won't work very well if it heals in that position and later hip replacement would be technically much more difficult. She wouldn't be expected to tolerate traction well with the usual high risks. So I would fix it. She's very osteoporotic and my goal would be restoration of bone stock for later or simultaneous total hip replacement depending on how bad the articular surface appears.
I would try to keep anesthesia/operative time down to decrease the chance of medical complications - at her age, even though she appears healthy, she is probably much more fragile than the average 20 year old. I would accept some minor joint incongruity to get her out of the operating room faster. We've been starting these patients on Fosamax hoping to improve bone quality.
Date: Thu, 15 Jun 2000 11:25:37 -0500
From: Adam Starr
I agree with Chip - we need a CT to better evaluate the injury. Telling us how long it's been since she was injured will help, too, since the operations that involved limited incisions, limited dissection, can become very difficult if you wait too long.
Far as I can tell, you have 4 options.
1. Do nothing surgically. Treat her with early mobilization with crutches, and expect her to get post-traumatic arthritis. Her femoral head will probably worsen the deformity when she gets up. You can count on a difficult total hip replacement at a later date. If you're lucky, her fracture will have healed.
I think bedrest until fracture union is a bad idea in any adult patient, but especially bad in an elderly patient. Decubitii and pneumonia can be very difficult problems.
There are no good studies on immediate mobilization of displaced acetabular fractures. The literature (Tile, Heeg, Matta, etc.) quotes periods of bedrest (+/- traction) ranging from 6-12 weeks. The OKU Trauma makes a similar recommendation. Still, I think bedrest is a horrible option for a patient like this.
2. Do an ORIF. David Helfet published a series of elderly patients treated with ORIF, and showed good results. The older patients seem to tolerate imperfect reductions better than younger patients.
I think many people would advocate doing this surgery through a single approach. Chip Routt, and David Helfet, and other authors have published series showing excellent reductions of complex fractures (which is what I think this is - I think it's an anterior column with a posterior hemi-trans...but we tend to call 'em "old people fractures" down here) through single incisions. So, if you choose to ORIF it, I'd go through one approach. (The CT will help you choose which one).
Reserve a unit bed if you choose to ORIF it. Expect to be frustrated with her poor bone stock. Strive to get the best possible reduction you can. I feel that, if you open her up, and expose her to all the risks of surgery, you should give her a shot at the benefits, too. Namely, a congruent joint.
3. Do a primary THR.
I have no experience with this. Dana Mears has a large series, and he is sold on it. I would imagine it would be next to impossible to get a press fit cup seated well into a busted acetabulum, even if you had stabilized it with plates and screws. I bet you'd wind up cementing the 'tab in place. I don't know that cement is necessarily bad in a 90 year old, though.
I think a primary THR would be a big operation. A 90 year old trauma patient will not act like a 90 year old elective total joint patient. The trauma patient will have a bloodstream full of bad humors, her lungs will act sick. So, beware. Anesthesia will be tricky. Reserve a unit bed.
***This next option is strictly experimental.
Do NOT try this at home.
Repeat, DO NOT TRY THIS AT HOME.
4. Transfer her somewhere where she can be reduced and stabilized percutaneously.
Using stab would incisions, her fracture could be reduced and stabilized with multiple cannulated screws.
The fracture reduction would not be perfect, but it would allow her to mobilize without further displacement, and would alleviate her pain. After fracture union, if she developed severe post-traumatic arthritis, a THR could be done. THR after percutaneous stabilization is much, much simpler than THR after failed ORIF.
Perc reduction becomes very difficult the longer you wait.
The surgery is technically very demanding. The fluoroscopic imaging is very demanding. The indications and complications of the technique are not yet well defined.
Don't try it at home.
Good luck.
Adam Starr, Dallas, Texas
Date: Thu, 15 Jun 2000 16:23:41 -0400
From: H C Cole
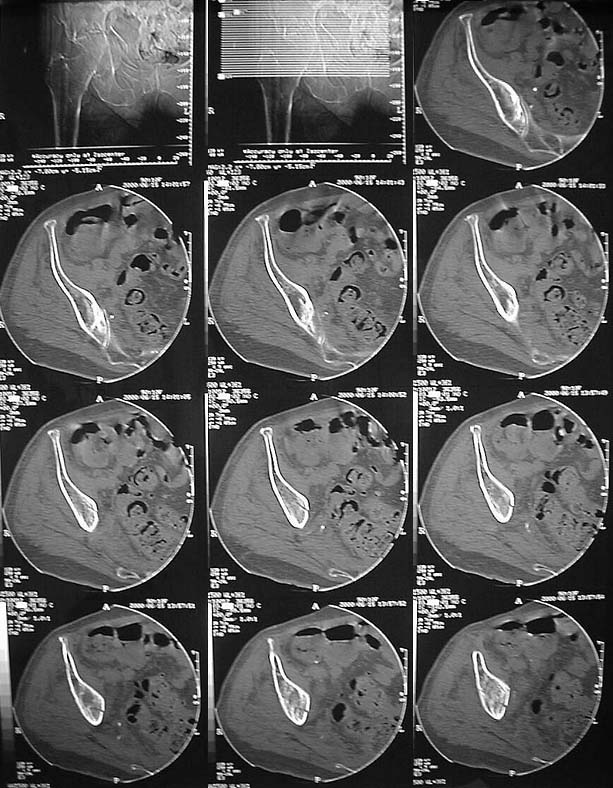
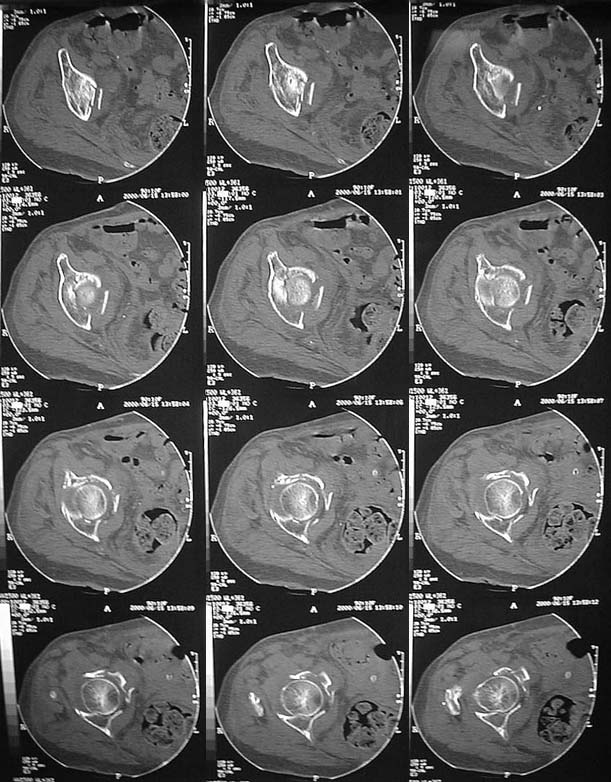
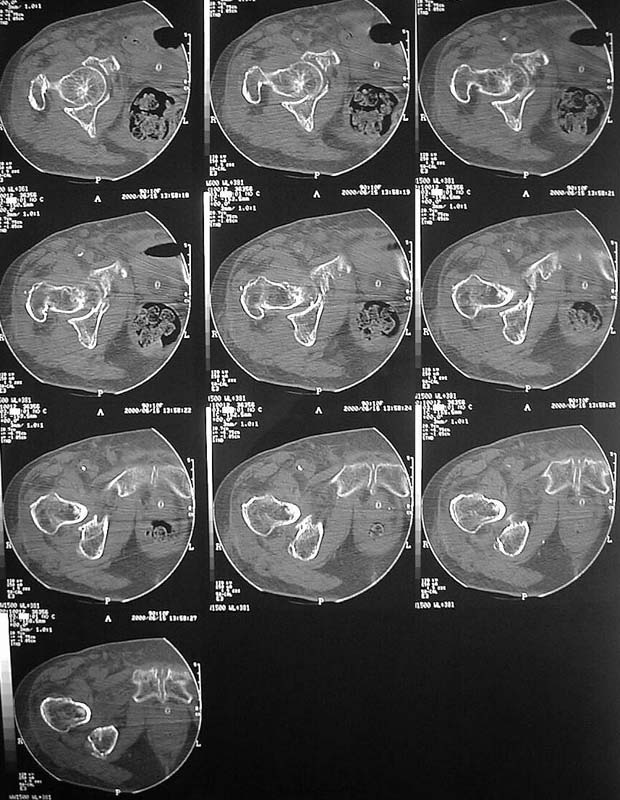
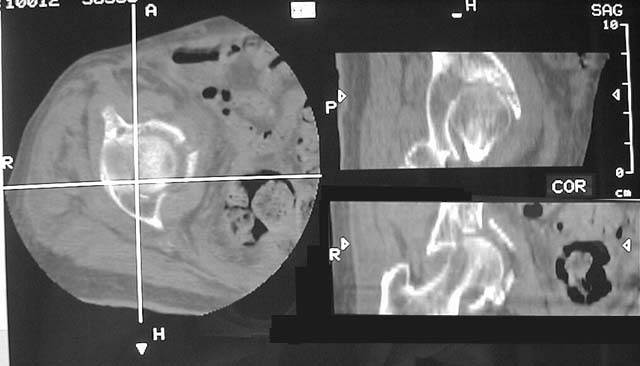
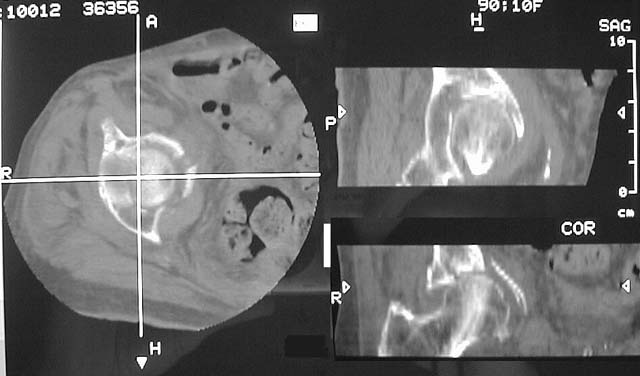
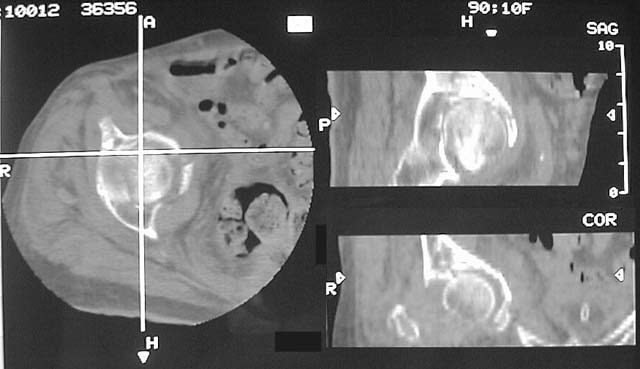
Thanks for all the input -- CT scans now up on Imagelist -- Had to use handheld camera -- Higher resolution views (xray and CT) available, if desired, but will be real bandwidth hogs for those of us with only dial up connections.
Fracture is now 5 days old.
 |
 |
 |
 |
 |
 |
H C Cole, MD, Steamboat Springs, CO
Date: Thu, 15 Jun 2000 17:10:57 -0500
From: Anglen, Jeffrey
In general, I tend to operate on these people no matter how old they are, if they are ambulators and the alternative is bedrest (few 90 year olds can stay NWB - they lack the strength to use a walker well). I've done at least a dozen nonagenarians with acetabular fractures.
The problem is I know of no way to support her head in a reduced position. You can pull it out lateraly from its medially displaced position at the time of surgery, but the anterior column and medial support is impacted and and the cancellous bone is crunched down and I don't know how to reduce it and bone graft it and hold it in place. The head will go right back medially. I've seen pictures of these spring plates bent over the brim and supposedly pushing against the medial wall, but I don't believe it ever really works.
Perhaps you could put some type of buttress along the quadrilateral surface through a Stoppa approach, but you still have to deal with the impaction of the articular surface. I think this is a case for primary total hip, and any other strategy is not only folly but risky to the patient.
Of course, I could be wrong.
Jeff
Date: 15 Jun 00 19:20:02 -0800
From: M.L.Chip Routt,Jr.,M.D.
she has a common fracture pattern for this population.
she has a comminuted low anterior column with several zones of impaction and a superolateral femoral head impression injury.
she'll benefit from accurate reduction and stable fixation, which can be achieved using predominately the iliac and extended pfannestiel (stoppa) windows of the ilioinguinal exposure. most of her acetabular impaction injuries can be accessed, reduced, and grafted using the stoppa interval. use ground cancellous allograft "paste" for support.
the cortical reductions are then routine. the quadrilateral surface plate as jeff suggests (anchored above the greater sciatic notch, slightly undercontoured, and extends to the pubic ramus) is extremely useful/mandatory in these situations...there are several technical tricks which facilitate their application. in these patients, you'll frequently find previously asymptomatic hernia or other anterior pelvic abnormality at operation so be prepared...most are seen on the preop ct if you look carefully at the surrounding soft tissues.
the femoral head impaction injury i have no trick for. i hope you have experience with these injuries since she's not routine and likely "won't take a joke". these patients do well, with durable joints. their medical comorbidities are problematic.
chip routt,md
Date: Fri, 16 Jun 2000 05:31:10 +0100
From: bruce meinhard
I would approach through an ilioinguinal incision, and I would recommend the publication by Dana Mears regarding the use of iliac (auto or allogenic) bone graft wired around the column to support the medial wall which looks fragile and risks protrusio of the femoral head.bpm
bpm