

Date: Sun, 14 Apr 2002 17:40:33
Subject: hip fracture dislocation
Dear trauma forum participants,
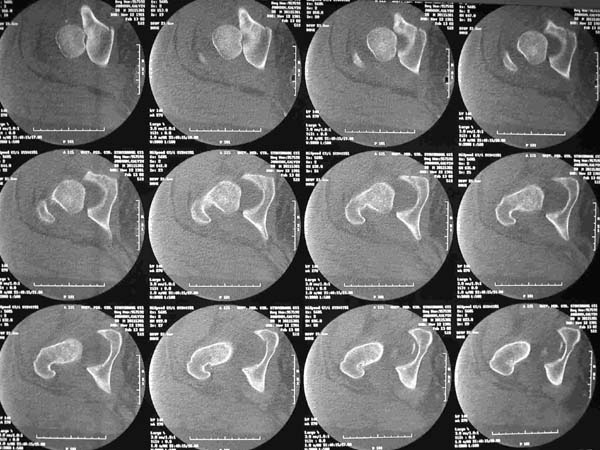
20 year old obese male presents after MVC. He was initially treated at an outside hospital but despite repeated closed reductions and traction the patient could not be held reduced. He was transferred to my hospital where we also attempted closed reduction. The patient reduced but was extremely unstable. Post-reduction xrays showed a nonconcentric reduction and CT scan showed bone fragments in the joint. The dislocation can be seen in the CT scan.
|
|
|
The patient was taken to the OR where an anterior approach was performed. Some small fragments of femoral head were excised and a small piece of acetabular wall was fixed. The fragment was so small, only one screw could be used to fix it. Torn capsule was repaired with #5 ethibond suture. An anterior column screw was placed to fix a nondisplaced transverse fracture.
 |
We then placed the patient in abduction traction which kept his joint reduced. The traction had to be discontinued because of skin breakdown and the inability to give the patient adequate nursing care.
The patient was taken back to the OR where a posterior approach was performed. Exploration of the joint revealed no loose bodies, no labrum or other soft tissue blocking reduction, no intra-articular hardware, anatomic reduction of the transverse component of the fracture (which was never displaced to begin with).
The patient dislocated again post-op. Because of the damage to his femoral head and instability I am considering hip fusion.
Comments on future management will be appreciated. Is his neck shaft angle contributing?
Nicholas Divaris, MD
SUNY Stony Brook University Hospital
Date: Sun, 14 Apr 2002 14:41:10 -0700
From: Chip Routt
First assure that it's not infected.
Your patient has an unusual (and unfortunate) anatomical and clinical combination...obese, a superolateral traumatic fracture dislocation, maybe some femoral head defect, and not much of a native dome to live in.
Did you examine the hip after fixation for residual instability? Do you have a film after surgery that demonstrates the head and dome congruent?
The upper CT images demonstrate a very peripheral and incomplete anatomical "dome" (see axial images 1,2,and 3)...some would call this acetabular dysplasia... but in this patient it's also in association with traumatic disruption of the all important local soft tissue envelope, hence clinical instability.
You'll see this "shallow" dome appearance frequently, if you look for it in patients with pelvic/acetabular CTs.
Before you attempt hip fusion, at least consider pelvic (and also proximal femoral) osteotomy for coverage/containment...get the proper films and make the drawings.
It's very difficult to contain the head in a shallow dome...but you already know that.
Don't miss an infection, which aren't always so obvious in the obese.
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
Date: Sun, 14 Apr 2002 9:50 PM EST
From: Bill Burman
>Before you attempt hip fusion, at least consider pelvic (and also proximal femoral) osteotomy for coverage/containment. . .
A similar recommendation can be found in this case report.
Marti RK, Kloen P., Chronic recurrent posterior dislocation of the hip after a Pipkin fracture treated with intertrochanteric osteotomy and acetabuloplasty. A case report. J Bone Joint Surg Am. 2000 Jun;82(6):867-72.
>...get the proper films and make the drawings.
Chip and others,
What about the role of stereolithography 3-D models in the preop planning of such cases ?
Date: Mon, 15 Apr 2002 06:50:22 -0500
From: Adam Starr
Hi Dr Divaris,
Obese patients are always hard to deal with.
I can't tell if he's reduced on the post-op AP film you included. Do you have any post-op Judet views? It might be easier if we had more films.
Do you have any films of where he is now? Maybe some traction films?
Adam Starr
Dallas
Date: Mon, 15 Apr 2002 14:13:05
From: Nicholas Divaris
Dear participants,
I actually had the patient planned for a proximal femoral varus osteotomy to see if I could get some more coverage of his head. I had all the implants and preop drawings available but then the patient developed a superficial wound infection with MRSA at the most proximal aspect of his anterior wound. This occurred under his pannus. We performed multiple I&D's and closed the wound. The wound looked clean.
I am considering fusion because I am concerned an osteotomy will become infected leading to a worse situation. Because of his size, I think the only way to fuse him is a cobra plate.
I have never seen an xray of this patient concentrically reduced. He is currently dislocated and cannot be reduced closed.
Nicholas Divaris, MD
Date: Mon, 15 Apr 2002 07:49:24 -0700
From: Chip Routt
His femoral side is not truly where the problem is. A femoral side osteotomy may augment stability, but the acetabular issue remains dominant. I refer you again to the native acetabular coverage, as discussed.
Sometimes we try to do what we know, rather than what our patients may need...sometimes that works.
Someone told me this, when you're in a deep hole - stop digging.
It sounds like you have plans based on more info than we have...so good luck-
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
{kind=link}