
Date: Wed, 8 Jan 2003 01:26:01 +0530
Subject: Floating Knee
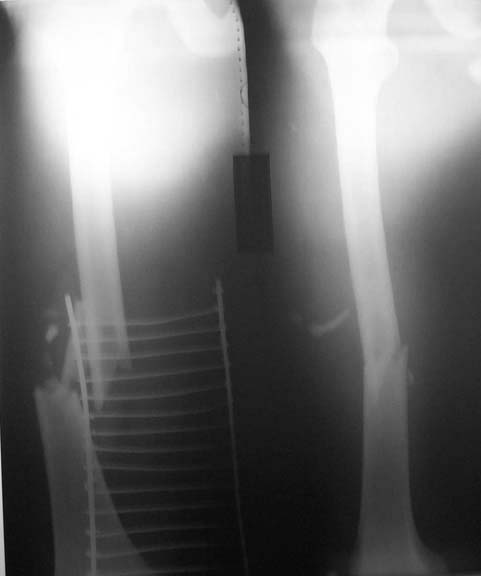
This patient was involved in a road traffic accident. Suffered total brachial plexus injury to right upper limb (clinically and investigation-wise pre-ganglionic) and fracture right femur and both bones right leg. He was referred to our unit as vascular injury since clinically and dopplerwise the previous centre could not get the distal pulse. However at our centre on resplinting the distal pulse reappeared. All fractures were grade II compound. Presented at 6 hours from injury. I am attaching the Xrays for you to see. I will be happy to know how you would stabilise these fractures. I will present what I have done after hearing the list opinion.
|
|
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Tue, 7 Jan 2003 14:26:08 -0600
From: Obremskey, William T
I&D both fxs, new drapes
Femur - retrograde reamed locked IMN
Tibia - antegrade reamed locked IMN
Close wounds if clean and able after debridement of nonviable tissue
IV anbx x 24-48 hrs
WBAT w/ A/P ROM of hip/knee
Union should be 98% w/ < 5 % infection
Bill Obremskey
Date: Tue, 7 Jan 2003 21:21:58 EST
From: Aobonedoc
One prep.
I+D fractures, close primarily.
Retrograde IM rod femur, statically locked.
Antegrade tibia rod, locked above and below, probably nonreamed.
48-72 hrs abx.
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005
Date: Wed, 8 Jan 2003 02:19:42 +0100
From: Dr. Josep M. Muñoz Vives
We would do the same procedure than Dr. Obremskey (retrograde nail + antegrade nail after I&D) except than we use an unreamed nail in the femur. We've found that 1 of the three fractures tends to heal slower than the other two (in the cases in which one of the two bones has a bifocal fracture).
Dr. Josep M. Muñoz Vives
Orthopedic Dept.
Hospital Universitari Dr. Josep Trueta.
Girona
Catalunya, Spain
Date: Thu, 9 Jan 2003 00:51:53 +0530
From: DR T I GEORGE
Thank you all for the response. I had in fact done what you had suggested. One of the leg wounds needed a flap cover which was done after 3 days. At this sitting cancellous bone graft was added to all the fracture site to enhance chances of bony union. With his total preganglionic brachial plexus injury we wanted to minimise chances for a delayed union/non union.
Three problems we used to face in these types of fractures:
1) The commercially available retrograde femoral nails were of maximum 25 cm length only.
2) The more proximal tibial fractures were not amenable to most of the commercially available nails because of the position of the curve in the tibial nail.
3) Very few companies were marketing solid nails that are available to us.
Fortunately for me all these problems were solved thanks to my involvement with SIGN an organisation known to most of you. SIGN nails can be used for antegrade and retrograde femoral nailing. They are at present available upto 38cm length. They are suitable for very proximal tibial fractures because of the position of the curve. They are solid. More than anything else they are dependable quality and US-FDA approved. The only factor beyond control and unenjoyable was that I had to start operating at about 2.00am.
I am attaching the post op (pre grafting) x-rays. Will be happy to get your comments/questions.
 |
 |
 |
DR T I GEORGE
Date: Thu, 9 Jan 2003 03:03:24 +0500
From: Alexander Chelnokov
Hello DR,
1)The commercially available retrograde femoral nails were of were of maximum 25 cm length only.
Why not use any available antegrade nail just insert it from below? The femoral fracture is high enough and doesn't require specific features of retrograde nails.
not amenable to most of the commercially available nails because of the position of the curve in the tibial nail.
IMHO any UTN imitation would do the job.
Very few companies were marketing solid nails that are available to us.
Why hollow nail would be unsuitable for the fracture?
involvement with SIGN an organisation known to most of you.
Pls give more details about SIGN and how the implants can be availble. THX in advance.
I am attaching the post op (pre grafting) x-rays.
Great! The tibia looks over-distracted a bit, so dynamization after 4-6 weeks would be useful.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 9 Jan 2003 08:33:20 +0530
From: DR T I GEORGE
Dear Dr Alexander,
You wrote: "Why not use any avalable antegrade nail just insert it from below? The femoral fracture is high enough and doesn't require specific features of retrograde nails."
I have not used the conventional femoral nail(AO design or GK type) in retrograde fashion. I suppose I will try it one day - initially on bone model. The SIGN IM nail is actually being used as a universal nail for antegrade and retrograde femoral nailing, tibial nailing etc. Some surgeons have used it even in the humerus successfully. Thus availabilty of SIGN nail seems to be a great weapon in our arsenal.
You wrote "IMHO any UTN imitation would do the job"
Quite possible I suppose. I have to look at it more critically.
You wrote " Why hollow nail would be unsuitable for the fracture?"
This case had a compounding wound at each of the fracture sites. Hence chances of infection are high. A hollow nail would have more surface area available for biofilm formation and persisting infection.
You wrote "Pls give more details about SIGN and how the implants can be availble. THX in advance."
You can get all the information from the web site: http://www.sign-post.org. If you need any further help in this regard I will be happy to help.
You wrote "Great! The tibia looks over-distracted a bit, so dynamization after 4-6 weeks would be useful."
Thank you. Will keep in mind your note on dynamisation.
DR T I GEORGE
Date: Sun, 12 Jan 2003 00:44:42 +0500
From: Alexander Chelnokov
Hello DR,
DTIG> I have not used the conventional femoral nail(AO design or GK type) in retrograde fashion. I suppose I will try it one day - initially on bone model.
Why? There is a lot of clinical examples of such usage.
DTIG> The SIGN IM nail is actually being used as a universal nail for antegrade and retrograde femoral nailing, tibial nailing etc. Some surgeons
Do you have a photo of the implant and needed equipment?
DTIG> This case had a compounding wound at each of the fracture sites. Hence chances of infection are high. A hollow nail would have more surface area
I am with you at this point though I have no experience with hollow nails. The only case of infection we've met at the series more than 150 solid nails was missed pre-existed cronic osteomyelitis.
DTIG> You can get all the information from the web site: http://www.sign-post.org. If you need any further help in this regard I will be happy to help.
Is there any detailed reference guide about the implant and technique online?
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 13 Jan 2003 16:02:40 +0530
From: DR T I GEORGE
Dear Dr Alexander
"How reliable is distal targeting device? What diameter is the locking screw?"
The distal locking devise is fairly reliable. But my problem is I am not that patient to rely only on this devise. I jump into using images if it is not smooth sailing. I have seen Dr Lewis Zirkle doing the most difficult locking without images.
If you notice pictures 10, 11 and 12 in the "Ind Tech manual presentation - (721 K)", you will see a devise (slot finding devise) being introduced through the nail before drilling the second cortex. This is the key to get the distal locking hole. The first cortex is drilled to a larger diameter. The locking slot is located using the devise mentioned and then through it the second cortex is drilled and then the locking screw is put in.
The locking screw is a stepscrew with two diameters. The smaller diameter engages the distal cortex and the larger diameter engages the proximal cortex. The drill bits used are .140" (3.56mm) and .250"(6.35mm). The diameter of the screws are 4.5 mm distal thread (I will let you know the proximal thread. Have to do some more looking up)
DR T I GEORGE