


Date: Wed, 21 Jan 2003 03:08:48 +0530
Subject: Compound femur fracture with cervical spine injury
Dear List members,
I would like to present this case to know how you would have managed this case. This young male adult was referred to us following a fall from a height. He had suffered injury to cervical spine and left femur. The previous centre could not get the distal pulses on the femoral fracture side.
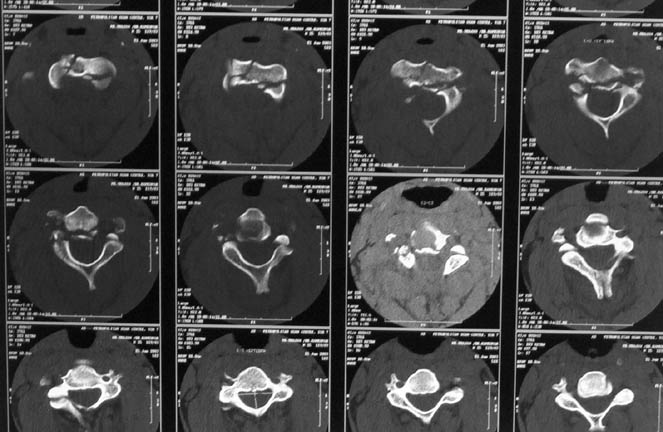
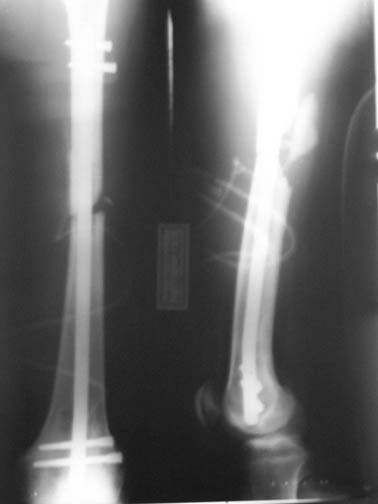
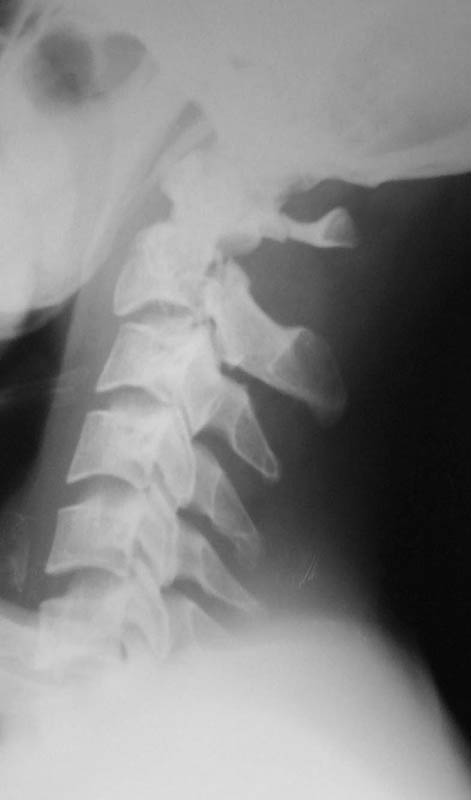
At our centre: Haemodynamically stable. Grade III compound fracture left femur with a wound anteromedially in the middle thigh through which the femur had come out. Distal pulse present. Cervical spine - C1 post ring fracture right side. C2 fracture body with listhesis. No canal compromise. No neurological deficits clinically.
X rays and CT film attached. We have put the patient on skull traction and posted him for debridement and proceed ----. What we have done I would like to present after the discussion.
Thanks in advance.
|
|
|
|
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Wed, 21 Jan 2003 22:36 EST
From: Bill Burman
Dr. George
2 links:
Bill Burman, MD
HWB Foundation
Date: Tue, 21 Jan 2003 20:25:09 -0800
From: Chip Routt
It's difficult to comment without quality films including the hip and knee.
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA
Date: Wed, 22 Jan 2003 15:36:16 +0530
From: DR T I GEORGE
Hip and knee normal. Will post the pictures at the earliest.
DR T I GEORGE
Date: Wed, 22 Jan 2003 08:17:08 -0500
From: James Carr
I like skull tx for the neck followed by bracing, and antegrade nailing for the femur. I would avoid retrograde thru the knee, since my dismal results with retrograde nailing have involved knee sepsis. If it is a long delay to initial surgery with lots of contamination, consider temp fix of the femur, followed by delayed nailing within 5-10 days. Finally, if the pulses were not bounding and symmetric, I would squirt his artery.
James B. Carr, MD
Palmetto Health Orthopedics
Date: Thu, 23 Jan 2003 00:30:38 +0530
From: DR T I GEORGE
Images of knee and hips.
 |
 |
DR T I GEORGE
Date: Thu, 23 Jan 2003 00:53:53 +0500
From: Alexander Chelnokov
Hello DR,
DTIG> and proceed ----. What we have done I would like to present after the discussion.
If all is done it seems to me it would be more relevant to discuss what your team has done. Looks like many people who would say something in case of advice request will keep silence in the "guess what we have done" context.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Thu, 23 Jan 2003 09:45:18 +0530
From: DR T I GEORGE
Dear Dr Alexander,
You wrote: "If all is done it seems to me it would be more relevant to discuss what your team has done. Looks like many people who would say something in case of advice request will keep silence in the "guess what we have done" context."
Your comment is quite reasonable. The reason I was holding back the done things were because, there will be some people who would not comment seeing what was done. Like the case : http://www.hwbf.org/hwb/conf/georg4/lenv.htm . This case I had posted after the patient expired. I held back the news of losing patient till the end. After the news of losing the patient was given very few comments came from OTA or orthogate or indiaorth. If I had given the news earlier then all the interesting discussions would have been lost. In the present case also we cannot hold on for discussion to do something because of the clinical situation. However these discussions do benefit me and hence these postings. I hope it benefits others also.
What we have done:
The case was taken for debridement and proceed with the skull traction on.
The anaesthetist did a orotracheal intubation though difficult with the
skull traction on.
I did a debridement and could get a satisfactory field for internal stabilisation. The options I had kept were Ex fix, antegrade nailing and retrograde nailing. Had to be prepared for an arterial exploration if required. The vascular bundle was lying exposed through the compounding wound and could get the pulse beyond the fracture site. For this purpose I used a radioluscent flat table and did not use traction table intra-op.
After debridement I did a retrograde nailing using a solid SIGN nail. I thought this gave me the best chance to do with minimal disturbance to the head end on a flat table where the patient was supine. Sepsis to the knee was a worry but since I was using a solid nail I was fairly confident that the two area of concern( the fracture site and knee joint) will be sparated and will not spread infection from one place to other.
 |
Post op patient is doing well but for mildly raised cpk secondary to muscle damage. This is settling.
The skull traction is being continued. My colleague, Dr K P Ramkumar, Chief of our Spine unit, said that the the cervical injury belongs to Levine type II and most probably it will be conservative management only. However he wants to repeat the x-ray on traction after a few days and do also a dynamic flexion and extension view. The need for surgical intervention will be decided after this. He also feels that patient has a subjective numbness of finger tips and mild grip weakness. According to him this indicates that the spinal cord had minimal trauma.
I will be out of station for a few days and will be able to continue the discussion only next week.
DR T I GEORGE
Date: Tue, 28 Jan 2003 00:59:32 +0530
From: DR T I GEORGE
The cervical spine x-ray done on traction in neutral, extension and flexion. Images attached. Request comments.
 |
 |
 |
DR T I GEORGE
Date: Sun, 16 Feb 2003 23:35:47 +0530
From: DR T I GEORGE
You will find attached the final follow up picture:
 |
I was disappointed that there was not even one comment after the cervical spine dynamic views were presented. Though there is instability, the CT picture showed that the body of C2 was totally comminuted and hence a decision to keep the patient in Halo was taken by my colleague in charge of the spine unit. After the consolidation of the body of C2 if required he will go through a formal C2-3 fusion.
What would have been the fate of this patient in this part of the world if we did not have the facility to do intramedullary nailing and CT assessment? Can we imagine this patient being kept on tibial and skull traction for over six weeks?? Definitely this will not be suitable for an citizen of first world. But I feel even for the third world citizens this treatment we gave cannot be termed a luxury.
 |
 |
 |
 |
 |
You will find attached in the remaining pictures the story of a young adult involved in a road traffic accident referred to us in shock. He had a major abdominal injury and had almost arrested before we took him up for surgery. After the abdomen was done I could boldly do the extremities thanks to the availability of nailing instruments and ventilator in the ICU. Of course he went through a rough period of rhabdomyolysis and an intensive critical care with daily battery of investigations which included electrolyte assessment, haemogram, blood gases, renal parmeters etc. Well yesterday I could shift him out of the ICU. Was his life and limbs saved through luxury of Western technology ?? I think it is only the availability of modern technology which has made us save these patients. Of course I envy the operation theatre I see in the Animal planet Channel. But with the limited infrastructure and not so high tech ICUs we can still save limbs and lives.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.