
Date: Mon, 16 June 2003 01:13:40 +0530
Subject: Post traumatic coxa vara and femoral shortening
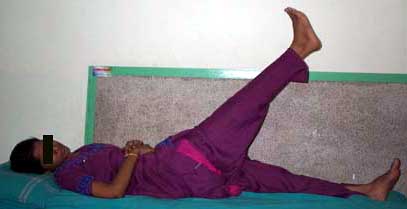
This 19-year-old girl was on long-term follow up after a major trauma (picture-01).
|
At the age of 9 years she was involved in a road traffic accident in which she suffered:
1) Closed fracture left femur midshaft,
2) Compound fracture right upper femur,
3) Compound fracture right side pelvis,
4) Degloving right lower thigh and leg etc.
At that time she was treated with care of wounds, external fixation of right femur, plating of left femur, skin grafting of right leg etc.
During the years of follow up it was noticed that she was developing shortening of right femur along with coxa vara. She was advised corrective surgery but came prepared for the same only now.
At present the problems to be dealt with were: coxa vara and femoral shortening (5cm) on the right side (Standing radiographs shown in pictures 02,03 and 04).
 |
 |
 |
The following procedures were considered:
Major problems that were envisaged were the following:
Prolonged maintenace of a fixator on the femur could give rise to lot of muscle irritation, pain and stiffness of the knee.
Femoral lengthening could go for a varus deformity during the lengthening process.
This case was discussed with Prof.Bhaskaran Nair and Dr. Vasudevan, RV Clinic for Ilizarov work, Palghat, Kerala, India. It was planned to do a valgus osteotomy and then lengthen over a nail, which could facilitate early removal of fixator and prevent deformity during lengthening. I have had good and useful discussions on this procedure with Andreas Papadopoulos MD, Orthopaedic department of Patras University Hospital, Patras, Hellas (GREECE).
The following plan was executed:
A supracondylar corticotomy was done on a flat OT table. A retrograde nailing of the femur using a SIGN nail of 280mm length followed this. The nail was locked near the knee but the proximal end was left unlocked.
The patient was transferred to a fracture table and performed a sub trochanteric valgus osteotomy, which was fixed using a bent heavy DCP.
Following this an Ilizarov frame was applied on the lower femur over the nail. The construct had one and a half ring above the corticotomy and one ring below the corticotomy. (Pictures 05 and 06).
 |
 |
One week after the corticotomy the distraction was started. After about a week there was no visible distraction taking place at the corticotomy and hence under anaesthesia distraction was checked using imaging. After making sure that distraction is taking place patient was returned to the ward and distraction continued(picture 07).
 |
Patient was discharged from hospital and distraction continued at home. After lengthening upto a difference of 0.5cm shortening (4.5cm lengthening) (pictures 08 and 09),
 |
 |
the fixator was removed along with locking of the proximal part of the nail (picture 10).
Total duration of fixator was about two months. In view of the osteotomy of the upper femur, weight bearing was delayed for six weeks and then encouraged to tolerable limits.
The knee movements though encouraged were not progressing till the fixator was removed (pictures 11 and 12).
 |
 |
However after the fixator came off, the range of movement increased significantly. The last review at about eight weeks after the fixator removal showed good regenerate at the distraction site and good progress of the knee movement (pictures 13, 14 and 15).
 |
 |
 |
I expect good further progress of knee movement.
Would welcome your valuable comments/criticism on this case.
I thank Dr Lewis Zirkle of SIGN and Dr Bill Burman of HWBF who encouraged me to present this case.
DR T I GEORGE.
Date: Mon, 16 Jun 2003 07:47:21 -0500
From: Frederic B. Wilson, M.D.
Dear Dr. George,
Why did you feel it necessary to place the retrograde IMN? Was there a delay in the regenerate?
Date: Mon, 16 Jun 2003 08:57:27 -0500
From: Alexander Chelnokov
Hello DR. George
DTIG> I will be thankful for your comments and criticisms.
Impressive case at all. congratulations! I hope knee motions will improved more. Why half-pins and wires were used simultaneously? If anyway wires above and below the gap were inserted, half-pins at same levels look not necessary, especially with the internal "guide".
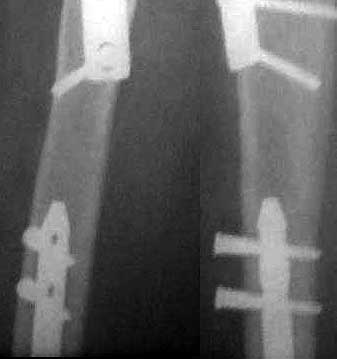
Proximal locking screws seem to be placed outside the holes. What targeting technique was used? Why this position was accepted?
|
THX for the interesting case.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 16 Jun 2003 22:01:11 +0530
From: DR T I GEORGE
Dear Dr Frederic,
Retrograde nail was placed for the following purposes:
1) To act as a guide during corticotomy distraction.
2) Leaving the distal holes locked and leaving the proximal hole unlocked in the initial phase allowed distraction to proceed without the fear of a deformity developing.
3) This guide should not have interfered with the proximal implant stabilising the valgus osteotomy and hence a retrograde nail was preferred.
4) After achieving the desired distraction proximal locking allowed removal of the fixator and thus all the wires and Schanz screws(half pins). This helped mobilising the knee better and also ensured that the regenerate will not collapse during further maturation.
In addition I may add the following. I had a discussion with Andreas Papadopoulos MD, Orthopaedic department of Patras University Hospital, Patras, Hellas (GREECE). He shared his unpublished finding with me. He felt that in experimental work when the regenerate is pierced by an unreamed nail, that further stimulates new bone formation.
Thanks for the interest in this case.
DR T I GEORGE.
Date: Mon, 16 Jun 2003 22:08:59 +0530
From: DR T I GEORGE
Dear Dr Alex,
You wrote: Why half-pins and wires were used simultaneously? If anyway wires above and below the gap were inserted, half-pins at same levels look not necessary, especially with the internal "guide".
I wanted to ensure adequate stability during the distraction process and hence added the half pins. Some of the wires were partly deflecting on the nail and hence this extra measure for security. Also my experience with Ilizarov work is limited and hopefully as time goes I may be more confident to go with wires alone.
You wrote: Proximal locking screws seem to be placed outside the holes. What targeting technique was used? Why this position was accepted?
I am attaching another view. This is not a good lateral but tells me that the proximal locking is in. The holes in this SIGN nail are oval and hence shows a gap in spite of the locking screw. Proximal locking was done using free hand technique under imaging.
 |
Thanks for the kind words on this case.
DR T I GEORGE.