



Date: Tue, 1 Jun 2004 20:52:37 +0530
Subject: Hip dislocation with femoral head fracture
From: tigeorge
Friends,
I request your opinion on the management of this case.
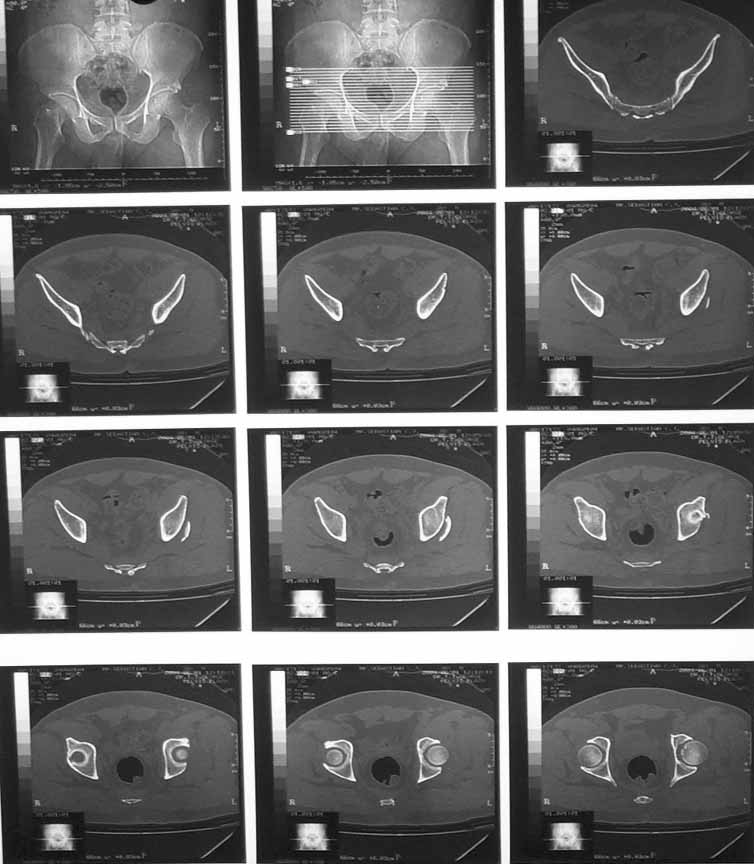
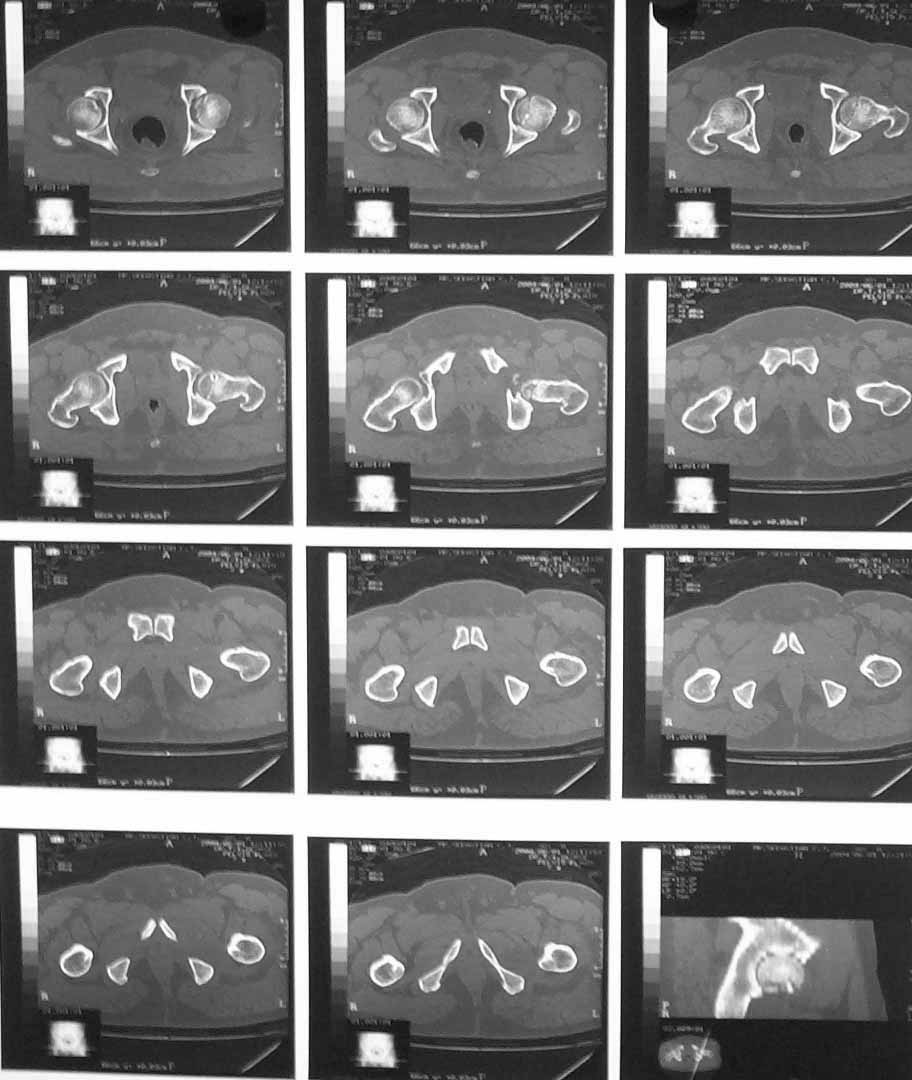
Middle aged adult hospital employee invoved in a road traffic accident. Suffered closed hip dislocation left side and fracture both bones right forearm(ulna compound) Underwent closed reduction of right hip and debridement with ORIF of forearm. Pre op X-ray showed acetabular rim fracture and post op X-ray showed a suspicious fracture line through the head of femur. One fragment of acetabulum seen displaced. CT done subsequently shows an undisplaced fracture through the head of femur with the acetabular rim fracture which is displaced.
My thoughts :
1) Posterior aproach to fix the acetabular rim and fix the head fracture simultaneosly. To fix the fracture from the trochanter the problem will be the width of the proximal fragment (less than 1.45 cm in the maximum width - measured from CT monitor). This means that I cannot lag the fragment from the trochanter. In fact if I try for that the fragment could get displaced. Other option was to consider fixation from the head while fixing the posterior lip and countersink the screw head.
2) Leave the patient on traction since the head fragment is undisplaced and hip is stable.
I would appreciate your thoughts.
Thanks in advance.
|
|
|
|
|
|
Dr. T. I.George
Head of Ortho Unit III
Little Flower Hospital
Angamaly, India
Date: Wed, 2 Jun 2004 17:05:45 -0700
From: Chip Routt
The head and wall fractures do not require operative management.
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
Date: Wed, 2 Jun 2004 19:21:24 -0700
From: Solberg, Brian, M.D.
We have treated 8 of these in the past 2 years using a digastric osteotomy with surgical dislocation as described by Siebenrock and Ganz. We have found it to be very useful in acessing the head fracture and posterior wall fracture simultaneously and unlike previous reports utilizing a standard Kocher approach, we have not had any cases of femoral head AVN. There is data from the European (and US) literature to support this approach as well.
I have also been burned by judging stability off the size of the posterior wall fragments alone. Our protocol is anyone with a documented dislocation and a Pipkin IV gets and exam under anesthesia to determine stability. We were surprized how unstable these fractures were even with minor posterior wall lesions and most end up with a surgical repair.
Brian Solberg, MD
Director, Orthopaedic Trauma
Cedars-Sinai Medical Center
Los Angeles, CA
Date: Wed, 2 Jun 2004 22:24:35 -0700
From: Chip Routt
Thanks.
I didn't track these for the first 5 or 6 years at HMC. There weren't many and they were confusing.
Over the past 9 years, I've operated on over 40 patients with femoral head fractures using an anterior exposure of the hip. These are unusual injuries at Harborview. Our operative technique has previously been detailed on this list. Two patients developed aseptic necrosis. Most of these patients were presented at the OTA several years ago by my partner Dr. Sean Nork including his patients as well. Maybe one day soon we'll finish editing the manuscript.
If you haven't had aseptic necrosis, just keep working and looking...it'll show up. It happens after hip dislocations...ask Bo...Bo knows necrosis.
Review your data/xrays. You should find that hip instability is seen in those patients with femoral head fracture and posterior wall fracture dislocations when the femoral head fragment is displaced...not in those where the head is truly well reduced after the dislocation is reduced. (Maybe you don't have any patients with the head fracture well reduced.) All of your 8 should have peripheral wall fractures...it's very rare to have a significant wall fracture associated with a significant femoral head fracture. The head needs enough wall intact to produce the head fracture. Big wall fractures correlate with small and caudal anterior head fractures, and vice versa. If that's not true in your patients, then you have a data set that should be submitted for publication now because you have a very unique 8 patients that we can all learn from!
It would be great if you'd share a similar example of a truly well reduced significant femoral head fracture with a peripheral wall acetabular fracture that actually caused hip instability. I've never seen one.
Do you use fluoro also to assess the hip EUA? If so, what views? How do you define the surprising instability? If it redislocates to prove instability, have you had a situation when it could not be reduced again closed...or the previous reduction was not achieved again? Are you sure that you've been burned by posterior wall size and instability correlations in patients with well reduced femoral head fractures...or has that just occurred in isolated wall fractures?
We learned from our femoral head patient series that if we accurately reduce and fix the head fragment(s), then the hip was stable to exam without wall reduction and fixation...but all of our walls were peripheral in location. For low comminuted anterior head fractures that mandate excision, the residual head defect after excision may cause hip instability when coupled with even a peripheral wall fracture...in these situations the wall needs reduction and fixation.
We also learned that the femoral fracture edges typically had chondral loss/comminution/impaction which frustrate anatomical reduction...these loss areas were almost always in the weight bearing area of the head...no surprise.
We also had a few patients with ectopic bone formation in/about the area of the rectus femoris tenotomy, so now we use routine indomethacin prophylaxis. But we used an anterior exposure and anterior surgical dislocation for fixation, we didn't use the fancy osteotomy and KL exposure...the lateral position is complicated/controversial for our polytraumatized patients.
The femoral head fracture in Dr. George's (unknown age or medical conditions) male patient is essentially nondisplaced, the hip joint is congruent, there is no joint debris, and the wall is peripheral. Leave it alone.
That's about all I know about that-
Chip
{kind=link}