

Date: Mon, 10 Jun 2002 20:43:53 +0530
Subject: Supracondylar Femur Fx with lymphedema
Requesting opinion on management:
68 year old gentleman injured in a road traffic accident. Sustained closed fracture left supracondylar region with intercondylar extension. Found to have bilateral chronic lymphaedema of legs with eczema. History of recurrent frequent breakdown. Has been a chronic smoker though stopped for 2years (smoked for almost 55 years of his life). Distal pulses not felt due to thickened skin but detected on doppler probe.Both knees show marked osteoarthritic changes. Patient ambulant till injury. Clinical picture and X-rayattached.
|
|
My thoughts and considerations: Any internal implant not desirable due to the presence of focus of infection in the same limb. Prolonged traction not desirable since this is an elderly patient who can develop secondary complications of recumbency. Short traction followed by casting again ruled out due to poor skin condition. That leaves me with only the option of closed reduction and Ilizarov ring fixator application. Will be happy to know the thoughts of other list members.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
Date: Mon, 10 Jun 2002 11:57:29 -0500
From: Gregory J Schmeling
What I see is a distal femoral fracture with a non-displaced intra-articular component and little metaphyseal comminution. The leg distal to the knee has bad skin, etc., but could be draped out of the surgical field. I do not have the experience with the Ilizarov to comment either way. I do disagree though, that an internal implant is not an option. I believe a small lateral incision could be made, the fracture reduced and a plate slid submuscular (MIPO not LISS). The proximal screws are placed percutaneously. A DCS could be used in this fashion but the introduction of the locking distal femoral plate makes this submuscular placement easier. I suggest another question;what will you dowhen he heals and needs a total knee replacement? Where would we be without tobacco to make our cases more challenging?
Gregory J Schmeling
Date: Mon, 10 Jun 2002 13:25:26 -0500
From: Adam Starr
Hi Dr George.
This is a difficult case. If ORIF is precluded due to skin condition, then you might consider a knee-bridging external fixator. I prefer a simple anterior ex-fix frame to the thin wire circular fixators.
You won't achieve anatomic alignment of the joint, but you will be able to maintain length and alignment, without the risk of wound sepsis.
Or, you could treat him in a cast brace. The nice thing about the cast brace is that it will allow immediate range of motion of the knee. Again, you won't get an anatomic reduction of the joint. The bones will stay lined up just like they are on the injury films, pretty much. But, they usually unite. In a 68 year old with major health problems, a supracondylar femur that is united, but a little crooked, may not be so horrible.
The bad thing about the cast brace is that you won't have access to the skin under the cast. So, the knee-bridging ex fix may be the best bet.
Good luck.
Adam Starr
Dallas, Texas
Date: Mon, 10 Jun 2002 20:51:50 +0200
From: Josep M. Munoz Vives
I think this is a case for retrograde nailing. Minimal skin incision. Enough distal bone to hold interlocking.
If you are worried about implant infection, in my hands external fixation pin tract infection is far more common than infection of internal implants, especially if they are placed in a minimally invasive fashion.
Dr. Josep M. Munoz-Vives
Orthopedic Surgery Dept.
Hospital Dr. Josep Trueta
Girona - Catalunya
Spain
Date: Mon, 10 Jun 2002 13:35:45 -0600
From: Thomas A. DeCoster
Retrograde nailing seems to me to be the best option in this 68 yo patient with distal femur fracture and below knee severe eczema.
TD
Date: Mon, 10 Jun 2002 14:08:48 -0700
From: John T. Ruth
Agree that nonoperative management will not result in a satisfactory outcome. I would favor closed manipulation with perc. screw fixation of condyles with placement of a retrograde IM rod. My preference for a rod is either the Synthes or Zimmer which allow use of a locking end-cap which will convert the distal-most locking screw into a fixed angle device. A femoral Ilizarov will be extremely problematic and will likely result in chronic drainage from the pin sites due to the lymphedema. No good solutions, but I would favor surgery over no surgery and an internal implant over and external fixator.
Date: Mon, 10 Jun 2002 18:04:52 -0400
From: James Carr
From what I can see, the knee is very arthritic, and his skin is poor below the tibial tubercle as you stated. The skin around the knee looks fine. I would favor retrograde femoral nailing. This could be done percutaneous, or with midline approach. If locked retrograde nailing is not available, I recommend rush rods. You don't necessarily need to fix the condyles. This could be done percutaneously, and likely will get him out of bed. I favor traction over Iliazorov. I find the dangers of traction tend to be underlying medical problems, and poor nursing care rather than the traction itself.
James B. Carr, MD
Palmetto Health Orthopedics
Date: Mon, 10 Jun 2002 23:19:46 +0100
From: Nuno Craveiro Lopes
Dr. George,
I advise a Ilizarov frame
Best regards,
Date: Mon, 10 Jun 2002 18:35:47 -0400
From: ebarrick
He might be a candidate for a primary knee fusion with a loooong femur to tibia IM nail.
Date: Sat, 15 Jun 2002 01:02:16 +0530
From: DR T I GEORGE
 |
 |
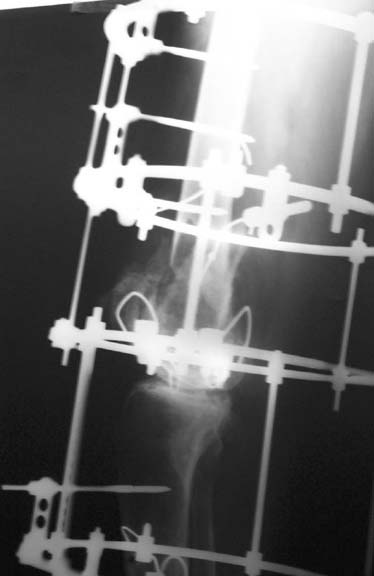 |
I have done closed reduction and Ilizarov ring fixator application in this case which I presented earlier. Patient is very comfortable. Skin has been opened only for K-wire / shanz screw introduction. Request your comments and opinions/criticisms.
Dr.T.I. George, Consultant Orthopaedic Surgeon,
Polytrauma, Microvascular Surgery And Hand Surgery Unit,
Metropolitan Hospital, Trichur, S.India.
{kind=link}