{kind=link}

Date: Fri, 18 Feb 2005 10:50:49 +0100
From: J.C. Goslings
Subject: Pipkin Type IV fracture
Dear list members,
Please share your opinion on the following case:
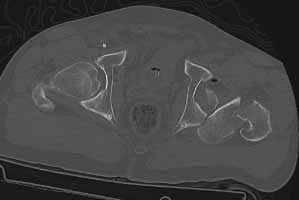
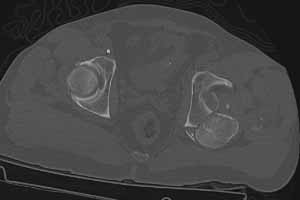
49 year old male, active speedskater, one year after MVC with multiple trauma and mild traumatic brain injury. Pipkin type IV fracture of the left hip. Same day ORIF through KL approach. No heterotopic ossification "prophylaxis". Day 7 wound revision for hematoma. Full weightbearing after 3 months. Full recovery except left hip function due to early severe HO. Function after one year: fixed ankylosis in 40 degrees flexion, 10 degrees exorotation. Patient frequently asks for attempt to improve hip function.
|
|
|
 |
 |
 |
 |
Questions:
Thank you,
Carel Goslings
Date: Fri, 18 Feb 2005 11:42:57 -0800
From: Chip Routt
Fracture patients are not the same as arthroplasty patients when it comes to HO.
We don't wait for metabolic inactivity as recommended for hip arthroplasty patients ... your fracture patients need chondral nutrition from movement ... don't wait ... when you see hip HO as clinically significant (usually the 2nd or 3rd month after surgery), early excision is indicated for fracture patients.
Sometimes the HO will cause progressive nerve deficit and you can't wait for maturation.
Use the CT scan to direct your exposure for excision ... operate wherever the bone is ... sometimes it forms remote from your initial surgery site and demands a separate exposure.
A 3D CT helps define the margins and direct the exposure(s).
Don't forget to manipulate the hip after HO excision while still under anesthesia ... take care because of the bone quality of the "normal" bone which has been unloaded for months by the HO mass.
No need for preop XRT ... you can irradiate after excision, directed at the area of previous formation/excision ... or use Indomethacin orally for 6 weeks.
Move the hip after excision with a CPM and consider a postop epidural anesthetic to provide comfort which should help maintain motion.
Protect weight bearing for 6+ weeks after excision because of the poor bone quality ... it takes a few weeks to restore.
Thanks-
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
Date: Fri, 18 Feb 2005 14:52:59 -0500
From: Anglen, Jeffrey O
Sometimes pre-operative irradiation is easier, if your rad Rx facility is not on site and transporting a fresh post-op patient is a problem. Just Beware the last minute OR cancellation, in which case the rads are wasted (unless you can get back on the schedule within 24 hours) and you can't buzz the same tissue twice.
JOA
Date: Fri, 18 Feb 2005 14:21:34 -0600
From: Sam Agnew
RE: Pipkin IV fracture dislocation-with associated femoral neck fracture. Now with Class IV heterotopic bone and dysfunction.
Question 1: Timing?
I don't believe that waiting until your surveillance studies normalize is
a prudent choice, waiting in cases of Class IV ossification tends to promote
cartilage degeneration from the prolonged immobility.
I would vote for early (earlier) intervention.
Question 2: Pre operative Irradiation
That would depend entirely on the approach(es) that are to be utilized for
the excision and exactly what procedure you are committed to- at a year
I would suspect that arthroplasty would be likely despite being a speed
skater.
Question 3: Approach?
For excision of Class IV HO and sparing the femoral head if that remains
an option I would say that based on your current CT scan that a dual approach
tactic would be necessary - Kocher
and Modified Smith Peterson.
Position in true lateral for KL
approach and can convert to semi-lateral for SP. Through either one
could perform the Arthroplasty if head/cartilage viability was questioned
on intraop evaluation. Post OP irradiation-our team prescribes single dose
750 mRad on post op day #1. Followed by indomethacin
and possibly diphosphonates as adjunct with head salvage procedure being
performed.
Good Luck, send pictures of him skating post op, cheers
Sam Agnew, MD, FACS
Date: Sat, 19 Feb 2005 0:6:30 AM EST
From: Bill Burman
Re the use of indomethacin for HO prophylaxis, what about this study?