Date: Sun, 2 Sep 2007 17:38:41 EDT
From: Gavin Pereira
Subject: Denis Type 3� Sacral Fracture
Dear Colleagues,
I am sending this case on behalf of a colleague of mine from another hospital in the UK.
The story sent to me so far.......
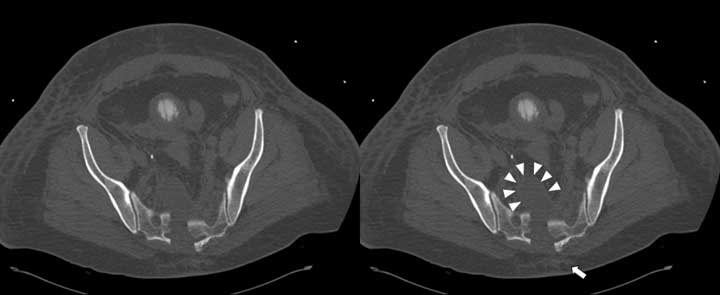
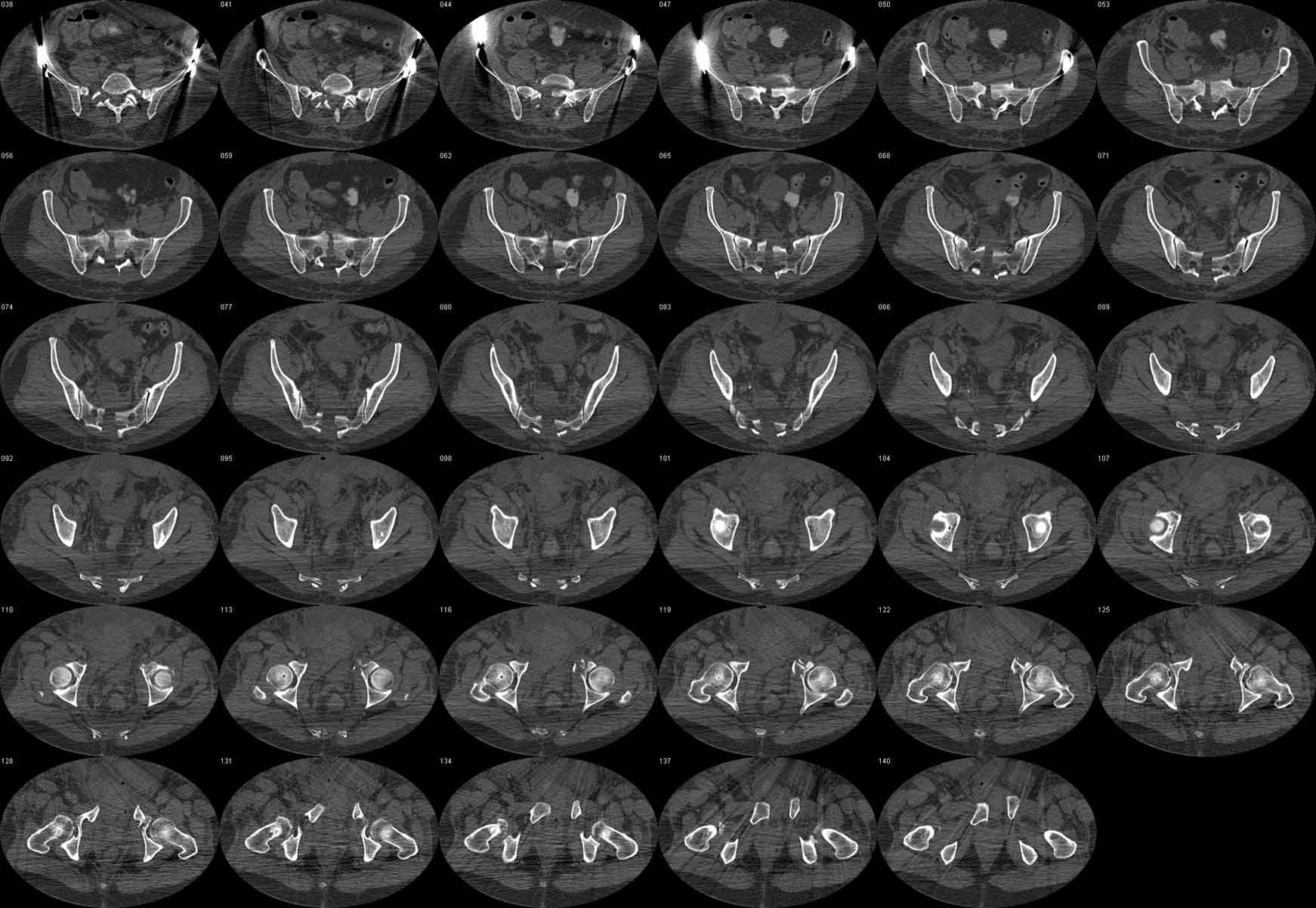
On 9.8.07, a (very large) 50y male motorcyclist came in with significant exsanguinating pelvic injury�. No further details on mechanism. Wrap->Embolisation->Ex-fix. Unfortunately, the rectal tear was missed (approx 24h, and has colostomy), as was what appears to me to be a bladder neck disruption (over a week). Not surprisingly he is septic. Has right lower anterior abdo wall sepsis - debrided and vacced. Urine now draining via surgically placed urethral catheter. Appears to be improving but still very sick. I am told that he could move his legs prior to intubation. I am trying to find out whether there were any meaningful perianal neurological findings� recorded.
Scans 3D and axial attached (these were done on 17.8.07). I have tried to window the axials to show the nerve roots best.
Click images to zoom in.
|
 |
 |
I am worried that trying to reduce the sacrum might squeeze the nerve roots between fracture surfaces. Even if they don't get pinched I wonder whether the canal should be decompressed from behind with all the oedema around. The possibility of sacral pressure sores in this sick chap over a posterior operation wound is unappealing. Ex-fix would make prone positioning difficult/impossible. These are just a few of the tricky thoughts bothering me about this.
I think prone would be difficult unless the ex-fix comes off. Also, I have now got his original admission scan which appears to show a bit of closed degloving under the sacral skin.
He is waking up a bit and he appears to be moving his legs. Sphincter-wise the anal shincter was apparently torn and the bladder neck is disrupted I think so we may never know his true continence.
Do you think the sacrum might throw out enough callus to stabilise sufficiently? As the fracture goes into the disc space I guess that vertical displacement is unlikely.
Many thanks,
Gavin Pereira
MBBS, FRCS(Eng), FRCS(Orth)
Consultant Orthopaedic and Trauma Surgeon
University Hospitals Coventry and Warwickshire
Clifford Bridge Road
Coventry CV2 2DX
UK