

Date: Mon, 18 Jun 2001 23:02:36 +0300
From: Armin Heiman
Subject: Osteochondral fragment
Dear All !
I would like to ask Your advice about the next case.
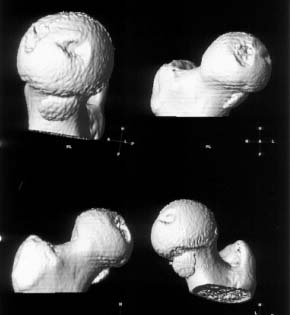
22 yrs man , semiprofessional( he earn some money from playing) basketball player got suffered in car accident.He had hip joint posterior luxation ( Pipkin 4) with little acetabular roof fragments ( nondisplaced) and anterosuperior abruption fracture of the head of the femur.
Additional injuries were severe face wounds. Emergency manipulations were reposition of the hip luxation under the radiologic control and wounds care. After reposition the CT scan was made. We found 2x3cm wide and 0.5 thick OCH fragment outside the joint surfaces , under the caput. The traction was applied.
|
|
|
What will be your suggestion for the free OCH fragment.
Armin Heiman
orthopedic surgeon
Estonia
Date: Mon, 18 Jun 2001 17:18:08 -0500
From: Adam Starr
Hi Dr. Heiman,
This is a tough case.
Everything about it is difficult. Choosing the approach is hard - do you use a Kocher? Or an anterior approach? I've used a Smith-Petersen approach, but it can be hard to see and hard to reduce the fragment using a Smith-Pete. With a posterior approach it's hard to obtain and judge reduction, and hard to get your screws centered in the fragment. If you decide to fix it, I think I'd vote for an anterior approach. But, I don't know what approach YOU are most comfortable with, or the best at. What I pick might not work for you.
I don't know what chance ORIF has of working. I'm not sure you can get the piece to heal very well. It's markedly displaced, almost certainly avascular. It looks pretty thin.
If you decide that an ORIF is likely to fail, then I wonder if the treatment you've chosen - reduction, traction, protection of the hip - might not be the best option? At least that way he won't have to accept the damage done by the surgical approach, in addition to the damage caused by the fracture.
But, if you decide to open and repair it, hopefully you'll discover a strip of periosteum from the femoral neck still attached the piece. In that case, the piece might still be viable, and might actually unite before it falls apart.
Good luck. Keep us posted on your decision.
Adam Starr
Dallas, Texas
Date: Mon, 18 Jun 2001 17:18:37 -0500
From: Steven Rabin
i'd like to see post reduction x-rays to assess congruency of the reduction including AP & both Judet views. If the fragment is truly small, and extra-articular and the joint is stable, probably nothing needs to be done with the fragment, but i'd like more views! thanks
steve rabin
chief ortho trauma
loyola university
maywood, Il
Date: Tue, 19 Jun 2001 06:46:28 -0700
From: Chip Routt
At least try to fix it, he's 22 years old-
Please don't use an exposure that you're "comfortable" with. Rather, use the correct exposure - one that allows fracture exposure and treatment.
Since the defect location is cephalad/anterior, and the fragment is caudal to the head anteriorly, you'll need an anterior surgical exposure...if you select a posterior exposure, you may be "comfortable"...but you'll be "sad" then "mad", since you won't see the defect. (see below)
You don't need the upper(iliac crest) component of a standard Smith-Petersen exposure. Instead, use only the lower limb which is necessary in order to expose, debride, reduce, and fix these particular anterior femoral head fractures.
So... position your patient supine, elevated on a sacral soft bump, prep and drape the entire flank and extremity, locate the skin incision distally from ASIS 10-12 cms directed between sartorius/tensor interval, preserve the LFCN branches, tenotomize the conjoined rectus femoris, use a T-shaped anterior capsulotomy (the upper limb parallels the intact anterior labrum and the lower limb parallels the femoral neck), remove the displaced fragment from the caudal anterior joint recess, irrigate the joint, prepare the dominant fragment on the back table -cleanse the clot and its debris, then if there is sufficient cancellous backing - drill a triangular peripheral pattern of the glide holes on the fragment, then use a figure 4 maneuver which delivers the head anteriorly from the joint, next reduce the fragment, then fix the fragment accurately (the reduction is infrequently difficult if there is peripheral comminution)...secure the fragment with buried long 2mm screws (these are typically special request items), use 2 or 3 of the glide holes for fixation, avoid screw convergence...the acetabulum is a perfect "spica cast" for the fixed femoral head, then replace the head into the joint carefully, a passive range of hip motion assures stability. Orthoganol xrays guarantee implant safety, irrigate the wound, repair the anterior surgical T shaped capsulotomy, repair the conjoined rectus tenotomy, avoid injury to LFCN branches.
Avoid excessive retraction on the tensor muscle.
If the fragment is without sufficient cancellous backing to be fixed, then remove it, debride the host site on the femoral head, drill the defect, and close as above.
Institute early active and passive hip motions. Protect his weight bearing 6 - 12 weeks.
For more info, see - Young Patients with Femoral Head Fractures. The Hip - Master Techniques in Orthopaedic Surgery, Vol. 9. Lippincott-Raven, Publishers, 1998.
See also - Swiontkowski MF, Thorpe M, Seiler JG, Hansen ST. Operative management of displaced femoral head fractures: case-matched comparison of anterior versus posterior approaches for Pipkin I and Pipkin II fractures. J Orthop Trauma. 1992;6(4):437-42.
That's it-
Chip Routt, M.D.
Harborview Medical Center
Seattle, Washington
Date: Wed, 20 Jun 2001 19:05:59 -0700
From: Chip Routt
What did you do?
Chip Routt, M.D.
Date: Thu, 21 Jun 2001 23:21:39 +0300
From: Armin Heiman
At least 3 week traction and when problems will arise concerning free fragment in future, Ill try to remove it arthroscopically.
Here are the missing postreduction views.
 |
 |
 |
Armin Heiman M.D.
Date: Fri, 22 Jun 2001 08:25:51 -0700
From: Chip Routt wow