




Date: Tue, 5 Dec 2000 10:33:53 -0500
Subject: LC3 Pelvic Fracture
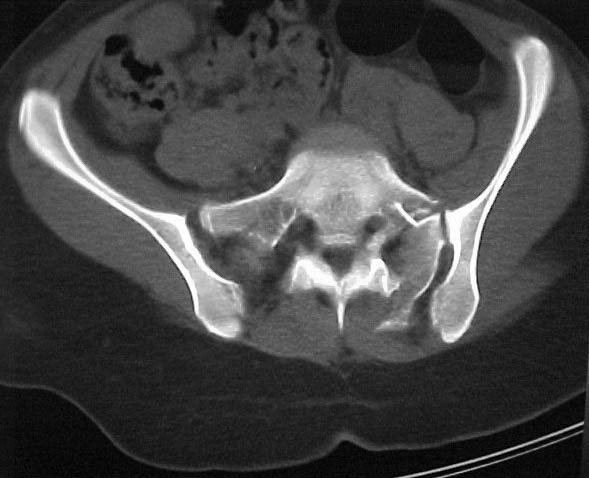
A 17 year old female involved in a car crash. Has a Type III lateral compression injury to her pelvic ring using the Young-Burgess classification. A windswept pelvis if you will. The images are included. There appears to be posterior displacement of the left hemipelvis as well.
My questions - should this be operated on? How to go about reducing the left side (i.e. correcting the posterior displacement as well as impaction) ? and How to fix it (iliosacral screws: posterior plate, etc.)? Thanks all!!
Paul Koerner
|
|
|
|
|
|
Date: Wed, 6 Dec 2000 12:53:04 -0500
From: Clifford B. Jones, M.D.
Fx/Injury Evaluation:
Impression: unstable, requires reduction with stabilization, will continue with continued deformity if not stabilized
Options:
1. Rt partially threaded perc SI screw (risky with dysmorphic anatomy) followed by derotational femoral distractor placed through iliac wings and finalized with Lt fully threaded perc SI screw (again, risky with dysmorphic anatomy, even riskier if sacrum not fully reduced)....followed by anterior stabilization of perc retro rami screws, anterior plating, or ex fix.
2. Posterior approach with open distraction, derotation reduction of Lt sacral (+/- foraminal decompression) fracture followed by posterior tension plate fixation (3.5 DCP bent over the PIIS) of both sides of pelvis...better idea with less risky approach to neural anatomy, but increased risk of posterior soft tissue irritation, infection, and prominent hardware.
3. Placement of 20 lbs Lt distal femoral skeletal traction for 4-6 weeks along with anterior iliac derotational external fixator application
Date: Wed, 6 Dec 2000 08:36:42 -0500
From: Agnew, Samuel G.
Dear Paul
Thanks for submitting your case to the forum, I am sure you will soon be toxic with recommendations that you will have to filter through. I would like to offer some rather elementary advice: Your patient needs to have appropriate inlet and outlet films adjusted for her anatomy;i.e.,she appears to be somewhat lordotic and that would require the gantry angle to be adjusted with each view. The same would be true for the CT scan it appears as though the angle of the gantry is tangential to the slope of the sacrum (sacro-horizontal line if you will) and that gives a distorted view of the posterior ring injury.
Cliff Jones gave you ideal insight into the problems with upper sacral segment dysmorphism and the problems this poses, and his recommendation list is quite complete.
The other issue is temporal, how far out from her injury is she now?, as impacted injuries such as this in someone her age tend to become immobile rather quickly in my experience, and if her nerves are molested on injury they won't like you very much at surgery if excessive force is necessary.
Finally, what type of equipment/experience do you have at your facility/faculty in dealing with this particular problem and the reduction/assessment maneuvers therein?
Good luck and thanks for contributing to the forum it gives Bill Burman and Allen Jones something to do.
{kind=link}