



Subject: Hand/Wrist Abrasion Injury
Date: Wed, 12 Jun 2002 14:38:27 +0300
From: Alo Kullerkann
Dear Members,
Please give your opinion in following case:
Four days ago 40 y/o female suffered in MVA. She was pedestrian and was droven over by drunken driver. She hooked underneath the car and was dragged by car 498.5 meters (police data). She got a severe friction of right wrist and arm, friction of face, left orbital fracture and both thigh and abdominal burns of III degree, about 10% caused by hot exhaustion pipe, also some friction burns.
At presentation arm debridgement was done and wrist was stabilized with 3 K-wires. There was complete loss of extensor tendons, distal third of dorsal pole of radius was grated away, proximal row of carpals was almost gone, loss of fifth MC and half of fourth MC.
3 days later a vascularised latissimus dorsi muscular flap was done, which is planned to cover with STSG after 5 days.
|
|
|
|
Any thoughts are welcome. Not to mention there is definitely not enough experience with that kind of injury.
Best regards,
Alo Kullerkann, MD.
Date: Wed, 12 Jun 2002 17:52:39 +0530
From: DR T I GEORGE
Dear Alo Kullerkann,
We do have similar problems on and off and usually we do a staged reconstruction. I think you have done well so far. In my centre the only difference is that we might have attempted a primary free flap cover if the conditions of the patient allowed. I would suggest the following:
1) Amputation of the little finger and as suggested by your Plastic surgery
colleagues use the skin where it is more useful.
2) Once the flap is settled and your microvascular surgeon is happy to allow
manipulation, then remove the k wires and change the wrist to a more functional position
with more extension. It will need to be stabilised with an external fixator at this
stage. At this time add cancellous bone graft to the wrist through the flap so that the
wrist will be fused in a functional position at the end.
3) Start passive mobilisation of the fingers (both IP and MCP joints) at the
earliest.
4) Once the tissues heal satisfactorily then you can start more active physiotherapy
to keep the fingers supple.
5) After all the fingers are supple and wrist stable the only task for you will be
extensor reconstruction. This can be done by using bridging fascia lata graft between
the proximal extensor muscles or doing a tendon transfer from the flexor side like in
radial nerve palsy. The donor tendons can again be lenghtened using fasia lata. I would
prefer to start passive mobilisation early but active mobilisation after three weeks.
Quite a challenging job but can get satisfactory end result with persistent work. Warn the patient that the whole process is going to take time and will need multiple staged procedures. If the patient is not co-operative or understanding, then the task will be Herculian(It is already tough).
Best of luck.
DR T I GEORGE,
Consultant Orthopaedic surgeon,
Polytrauma, Microvascular Surgery and Hand Surgery Unit,
Metropolitan Hospital,
Trichur, South India.
Date: Tues, 9 July 2002 12 noon
From: Bill Burman
A late submission of a similar albeit less extensive injury. This case presentation is derived from a lecture on Upper Extremity Tendon Transfers by Dr. Peter Stern of Cincinnati and is part of the Maine Orthopaedic Review Lecture Archives. Dr. Stern has given permission for its use as part of this OTA List discussion of soft tissue avulsion injuries.
----------------------------
Dr. Stern: How about tendon grafting? There is a very narrow range
of
indications for tendon grafting is indicated. There must be an intact proximal
motor from which the native tendon has been avulsed.
 |
 |
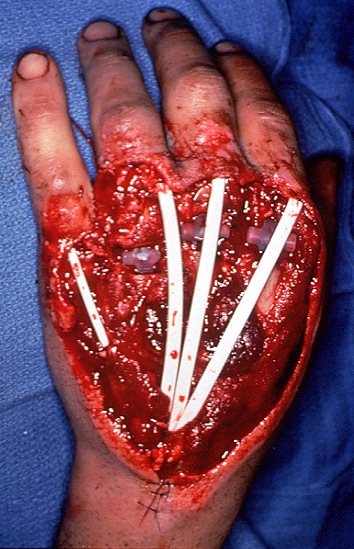
An example is a patient who had a degloving injury to the dorsum of his hand. There are multiple problems. There are fractures of the metacarpal heads of the index, middle and ring fingers. The extensor tendons, as well as the dorsal soft tissue coverage, are missing .
While it is possible to cover all this with skin graft, there will be adhesion problems of flexible joints and mobile tendons. Therefore, full-thickness flap coverage is required to secure a decent result.
 |
 |
In this case, we placed temporary silicone Hunter rods and silicone spacers in the metacarpal heads of index, middle and ring digits prior to covering it all with a conventional two pedicle groin flap.
 |
The flap was detached about three weeks later. Three months later the rods were replaced with tendon grafts originating from the native motor and inserting into the extensor hood over the MP joint.
 |
 |
This patient actually demonstrates a spectacular result. These images were obtained 15 years later. He has full MP extension and reasonable flexion of his MP joints.
----------------------------
Date: Thur, 11 July 2002 12:18:23 +0530
From: DR T I GEORGE
I have not used silicone rods so far. Maybe it's non availability could be a factor in not using it. I would not say I am totally unhappy without it for later tendon work.
DR T I GEORGE,
Consultant Orthopaedic surgeon,
Polytrauma, Microvascular Surgery and Hand Surgery Unit,
Metropolitan Hospital,
Trichur, South India.