

Subject: Hip Pain
Date: Wed, 11 Dec 2002 10:20:52 +0100
From: Alo Kullerkann
Dear Members,
I would like to ask your opinion on following case:
16 y/o boy, involved in karate in national level, complains pain in his hips (dex(Rt)>sin(Lt)). He has had 2-3 blocking episodes in right hip which resolved with rest and pain medications. Passive ROM is excellent (streching in karate) with no pain. He feels moderate pain during excersise and after.
What could be the diagnosis and is there any form of treatment?
Boy asks me if he can continue with karate, but I do not have a grounded answer...
Thanks in advance,
|
|
 |
 |
Best regards,
Alo Kullerkann, MD.
Date: Thu, 12 Dec 2002 11:52:25 -0500
From: Djoldas Kuldjanov
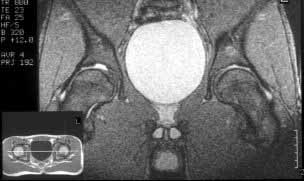
I believe this patient has anterior hip impingement caused by a retroverted acetabulum. This is seen on the submitted AP x-ray by observing the overlap of the anterior wall and posterior wall. In an acetabulum with "normal" version, the anterior wall shadow meets the posterior wall shadow at the superio- lateral aspect of the acetabulum, and they do not overlap as you follow the lines inferiorly. In an acetabulum with retroversion, the two shadows cross over the femoral head, making a figure 8 pattern.
To further confirm this, obtain a full AP pelvis film and a false profile view of both hips. In addition, the patient has an element of hip dysplasia, seen by his decreased center edge angle. On physical exam, his pain will be reproduced by hip flexion, adduction and internal rotation, when the anterior surface of the femoral neck impinges on the anterior labrum and wall. An MRI may show hypertrophic changes in the femoral neck. I also recommend a gadolinium MRI hip arthrogram to ensure there is no significant labral pathology.
Recommended treatment would be to perform a periacetabular osteotomy, making sure the retroversion is addressed in addition to giving more coverage laterally for the dysplasia. Any labral tears seen on MRI can be addressed before the osteotomy by a capsulotomy and excision of the labral tear and trimming anterior aspect of the neck, followed by capsular repair or patient has to live with pain.
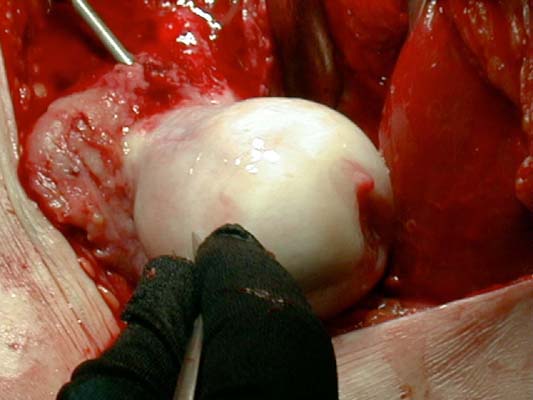
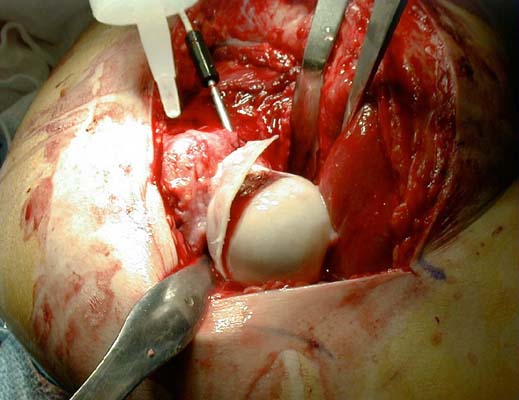
Here are some pictures from a case where the femoral head was surgically dislocated and trimmed for acetabular and femur impingment syndrome.
 |
 |
 |
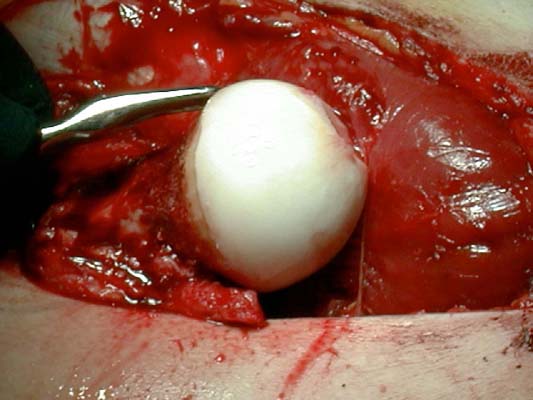 |
The technique is described by Ganz and Mast as a digastric approach (trochanter flip osteotomy) to the hip joint without destroying blood supply to the femoral head. The approach may also be applied to some acetabular fractures.
Djoldas Kuldjanov, M.D.
Associate Clinical Professor
Department Orthopedics.
Wayne State University
Date: Mon, 16 Dec 2002 11:53:35 +0100
From: Alo Kullerkann
Acetabular retroversion - so only it can be blamed for pain in hips? What about those holes in acetabulum - are they of no importance? T2 weighted images show them to be connected to joint cavity.
|
Patient has no positive signs for impingement. What about of blocking episodes - what come they from? Maybe there are some loose cartilage flaps at those holes?
Alo Kullerkann, MD.
Date: Fri, 20 Dec 2002 10:36:33 -0500
From: Djoldas Kuldjanov
"Acetabular retroversion - so only it can be blamed for pain in hips?"
Most likely - in my opinion.
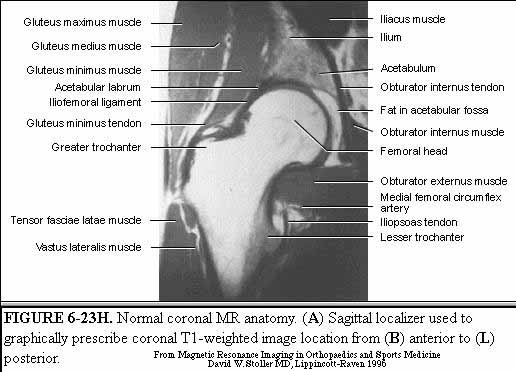
"What about those holes in acetabulum - are they of no importance? T2 weighted images show them to be connected to joint cavity."
My radiologist and I couldn't find holes in acetabulum. Perhaps you are talking about the acetabular incisura or notch. As can be seen in this image of a normal coronal hip MR from Stoller's text on MRI in Orthopaedics and Sports Medicine, the acetabular notch can have a significant extent into the weight bearing dome.
"What about of blocking episodes - what come they from? Maybe there are some lose cartilage flaps at those holes?"
Acetabular retroversion is a form of hip dysplasia which can lead to degenerative wear of the hip joint as manifested by joint space narrowing,irregularity and fragmentation as is seen in Reynolds et al Mar 1999 JBJSB article cited previously. Usually loose cartilage can be seen on MRI.
Djoldas Kuldjanov, M.D.
Detroit Receiving Hospital
Date: Mon, 23 Dec 2002 10:11:52 -0500
From: James Carr
I think the retroversion can produce symptoms as described. A hip arthroscopy will show you if there is local wear and tear, loose fragments, labral problems, and would not preclude later osteotomy. If you or the patient is hesitant about doing the big operation, the scope may provide some diagnostic info, and possibly some relief of symptoms.
James B. Carr, MD
Palmetto Health Orthopedics
{kind=link}