Date: Thu, 12 Jun 2003 09:51:32 +0200
From: Alo Kullerkann
Subject: Nailing after Ilizarov
Dear List Members,
Support is needed in next case.
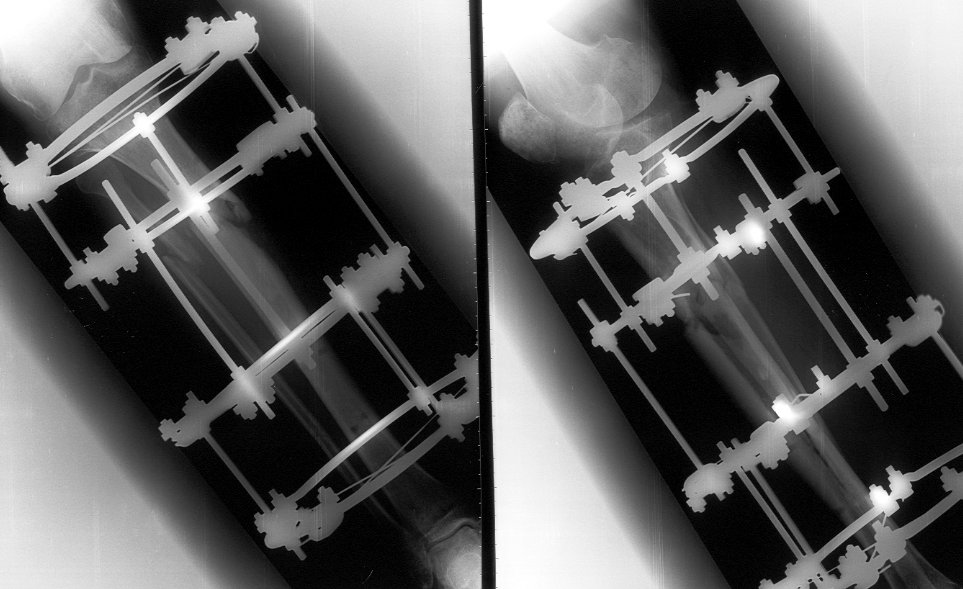
45 y/o male sustained in MVA 3 months ago. Had closed proximal third left tibial fracture. Initially treated in rural hospital where IM nailing was attempted but complicated with longitudinal tivial split down to tibial shaft to distal tibial metaphysis. Nailing was abandoned and cast was applied and patient was reffered to us.
We applied Ilizarov frame, which was performing nice until 1 month ago when patient started to bear full weight. Yesterday patient presented to us. Gross Ilizarov frame instability and fracture movement was detected. Patient has minor pain in FWB, pins are infection free.
|
My plan was to remove frame, apply cast for 2 weeks and then perform closed reamed locked nailing following 6 months PWB and then gradual FWB.
Today morning I presented my plan in my clinic and got lot of objections from my elder collegues like :
- this fracture is not suitable for nailing
- if you nail it you will split the fracture down to ankle
- this fracture will not heal if nailed
- after Ilizarov frame there is unacceptably high risk for intramedullary infection if nailed
And last but not least we (all) do not have enough experience in nailing of such fractures which is true. But there is nowhere patient to send. Wondering where the experience comes from if you do not try to get it?
Now I have to remove frame apply long leg cast for 2-3 months and then if not healing performe IM nailing.
WHY???
IMHO this fracture could be nailed. And reaming will act as internal osteoplasty. If I get axis straight and use distal locking first and performe backstroke technique I will get reasonable contact and some compression at the fracturesitee.
IMHO there is no problem even in nailing without delay after exfix if there is no pin tract infection.
IMHO this fracture will not heal in cast, if contrary there will be significant ankle and knee stiffness and muscle atrophy afterwords.
Please help!!! What would you do?
Does anybody know some specific references?
Alo Kullerkann, MD.
Date: Sun, 15 Jun 2003 15:34:16 -0700
From: Muhammad Amin Chinoy
I am no Ilizarov expert, but always thought that these type of complications are not only rare with use of Illazarov, but probably will respond to simply by readjustment annd retensioning of the frame. Any comments or thoughts?
Dr. M. Amin Chinoy
Date: Thu, 12 Jun 2003 19:37:58 +0530
From: DR T I GEORGE
Dear Alo Kullerkann,
I feel it will be quite safe to nail after a waiting period like couple of weeks in a support that will ensure good healing of pin tracts. Few tips: Use a nail with very proximal Herzog's curve. The AO design with low curve will not suit this fracture. Smith and Nephew has this design with proximal curve. GK also has proximal curve if I remember correctly. Solid nail may be better than hollow nail since ther is a potential for latent infection. If you have access to SIGN nails, both the above criteria are met in these. Only problem is that you cannot use a guide wire for the nail but it can be used for the reaming the removed with nail going in with image guide. Best of luck. ONLY WAY TO AVOID POST OR INTRA OPERATIVE COMPLICATIONS IS TO AVOID OPERATING!!!! But if you do not operate then the losers are the patients and your experience.
DR T I GEORGE.
Head of Orthopaedics Unit III
Little Flower Hospital, Angamaly
Kerala State, India
Date: Thu, 12 Jun 2003 16:07:19 -0500
From: Frederic B. Wilson, M.D.
Dear Alo,
I would be slow to abandon the Ilizarov, especially given your assertion that the pins are intact. The Ilizarov cannot work properly if it does not provide adequate stability. The bone cannot heal if it is kept distracted. I have attached a copy of your radiographs which I modified using Power Point and then saved as a jpeg file.
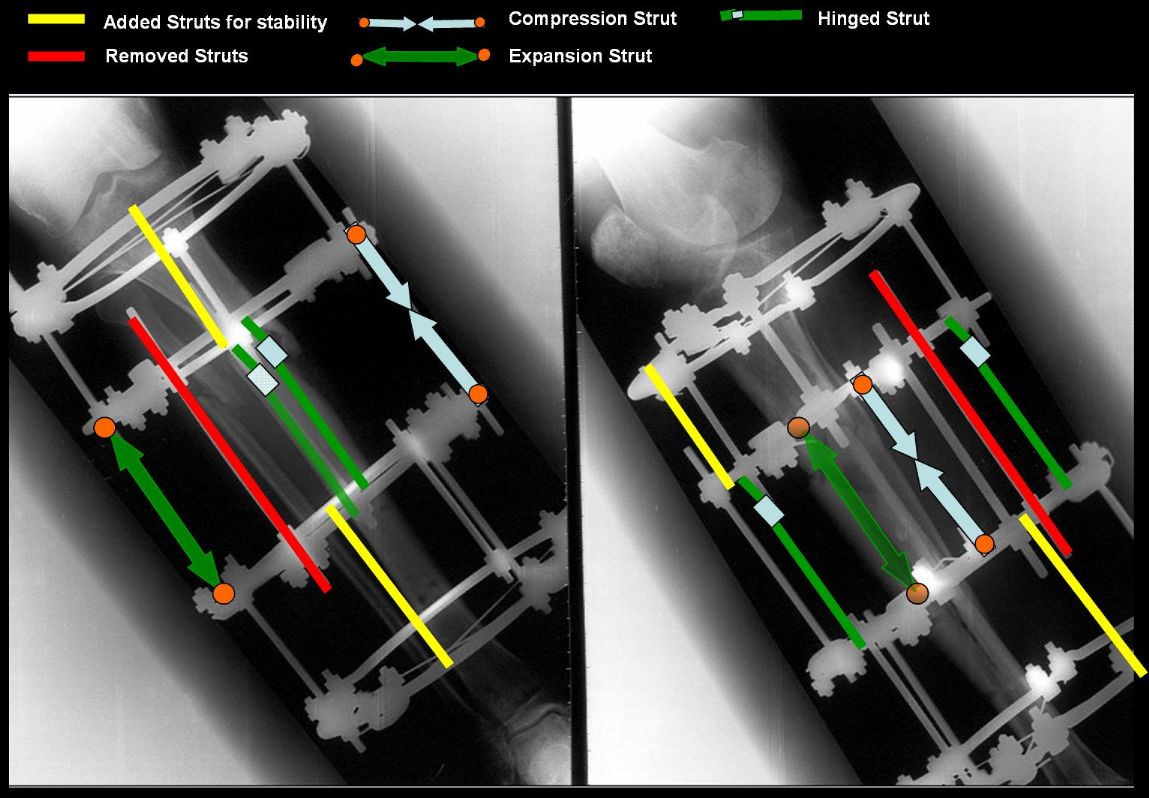 |
I would add a fourth rod to each of the top and bottom constructs and space the four rods in quadrants. Iwould then place a compression rod medially and a distraction rod laterally. Next I would place hinged rods as shown anteriorly and posteriorly. This will allow correction of the valgus malalignmennt. Once that is accomplished, the four rods in the middle segment can be converted to a straight compression construct to compress the fragments. I would perform these maneuvers in the order described to avoid impingement of the fragments if both compression and angular correction were attempted at the same time.
Please excuse the crude and hurried drawing but I wanted to get an answer off before you burned a bridge by removing the frame and nailing this fracture.
I would advise against conversion to an Intramedullary Nail for the following reasons:
1. Proximal fracture with osteopenic bone (disuse osteoporosis) is a recipe for possible fracture in attempting to insert the nail and make the corner .
2. Reaming will further compromise the bone by damaging the endosteal circulation. Unreamed nailing would be riskier given the bone quality.
3. Adequate biology is probably present at the fracture site which would heal given better stability and compression.
Finally, I would consider bone grafting after realigning and docking if it appeared that the fracture was not healing. I would ass wires or half pins as needed to further enhance fixation or if wires loosened.
One other thought. Do you find any irony in an American-trained Orthopaedist recommending the frame while you lobby for the Intramedullary Nail? Hmmm.
Frederic B. Wilson, M.D.
Assistant Professor
Trauma and Adult Reconstruction
Department of Orthopaedic Surgery
Tulane University School of Medicine
New Orleans, LA, 70112
Date: Fri, 13 Jun 2003 19:03:11 +0600
From: Alexander Chelnokov
Hello Alo,
AK> and then perform closed reamed locked nailing following 6 months PWB and then gradual FWB.
Why do you plan so long period of WB limitations?
AK> - this fracture is not suitable for nailing
Because of what reason? Just curious, because the pattern is definitely suitable for nailing. Too high? Or what they say?
AK> - if you nail it you will split the fracture down to ankle
Forced pushing of a thick nail to the underreamed canal may cause this, maybe.
AK> - this fracture will not heal if nailed
There is no rationale for such a verdict. As a rule it will. As exception - maybe, but there are options for this rare situation like dynamization, exchange nailing, bone grafting...
AK> - after Ilizarov frame there is unacceptably high risk for intramedullary infection if nailed
An interesting point. We now have more than 30 cases of nailing after ex-fix. About a half of them was acute exchange of fixators 1-11 months old. To our experience absense of clinical signs of infection makes nailing with minimal reaming safe. With 5 days antibiotic coverage no case of deep infection. Though we haven't used hollow nails.
AK> IMHO this fracture could be nailed. And reaming will act as internal osteoplasty.
In this case reaming barely looks mandatory - it is 3 months old, so dynamic locking should be used. Unreamed nailing can also be performed. In any case i would allow weight-bearing as tolerated.
AK> Please help!!! What would you do? Does anybody know some specific references?
I may send my recent abstract in Russian on the topic if it helps.
Best regards,
Date: Fri, 13 Jun 2003 19:06:08 +0600
From: Alexander Chelnokov
Hello Dr. George
DTIG> Use a nail with very proximal Herzog's curve. The AO design with low curve will not suit this fracture.
Why?
Best regards,
Date: Fri, 13 Jun 2003 21:28:19 +0530
From: rajesh
Re: using powerpoint to edit pictures
Fred,
That is a very neat trick. Never knew one could use powerpoint to edit pictures like this. Thanks for the tip. I have been practising on xray jpegs all evening now !
rajesh
Date: Fri, 13 Jun 2003 22:20:51 +0530
From: DR T I GEORGE
Hi Alex,
I was thinking to myself why there were no responses from people like you and Mangal Parihar (Ilizarov experts) for this case. .
You asked why the AO design with the low Herzog curve is unsuited for this fracture!
|
If you were to look at the X ray picture, the fracture comes close to the junction of upper one third with lower two third. In this anatomical location the AO design nail tends, not to allow an anatomical reduction and in fact may push the distal fragment to posterior displacement and distraction to an unacceptable extent.
Any comments from any hardline AO group members?????.
DR T I GEORGE.
Date: Sat, 14 Jun 2003 00:11:56 +0600
From: Alexander Chelnokov
Hello Dr. George
DTIG> I was thinking to myself why there were no responses from people like you and Mangal Parihar(Ilizarov experts) for this case.
:-) Just because i'm not an expert in internal fixation techniques. Apparently the case doesn't look too problematic for external fixation also, one may proceed with closed reduction, half-pin insertion and frame reassembly to make it more comfortable, and leave him for some months with full weight-bearing. But the two stage treatment looks to be a more attractive option.
DTIG> You asked why the AO design with the low Herzog curve is unsuited for this junction of upper one third with lower two third. In this anatomical location the AO design nail tends, not to allow an anatomical reduction and in fact may push the distal fragment to posterior
It still can be performed. IMHO the only limitation is that the proximal fragment must be have enough space for at least two screws.
See a recent example in a 76 y.o. female.
 |
Best regards,
Date: Sat, 14 Jun 2003 11:04:51 +0200
From: Alo Kullerkann
Dear dr. Wilson,
Thank you for excellent sketch. Actually frame supplementation was the first taught of mine too.
But I need to explain backround. We work with sets of Ilizarov what our hospital bought 15-20 years ago when we were enfolded in Soviet Union. Now when we have been independent country again for 12 years it is not popular to buy any implants from Russia. I am aware that there is on the market lots of fancy Ilizarov western analogues but those are still too expensive for us. So it leaves us with limited hardware and even those that we have are made of very soft metal - thats what sometimes can cause frame instability. Secondarily as we do not have abundant sets of sterile components offentimes we first assemble the frame, then sterilize it, then apply it on extremity. In this manner you have to have good bony alignement beforehand or you end up with malpositioning, like in case presented :-) The frame that was used in presented case was not technically so successful - three bars, wires not perpendicular to bone and not crossing in the centre of bone etc. But in addition the ! rings what was used come from ancient ages and did not have enough holes - 10 holes per circle. 3 take bars, 4 take wires, and it leaves 3 unused holes. This makes reassembling pretty tricky. So as I planed to nail this tibia I removed the frame and then got gold shower from elder collegues who decided best treatment to be long leg cast 2-3 months and then nailing again, which would be much safer this time as longitudinal split fracture would be united to that time.(?) Chances for upper fracture to heal are low anyway(?).
With my limited experience I would go for nail after 10 days of cast and if nailing fails then accurate Ilizarov again.
> you find any irony in an American-trained Orthopaedist recommending the frame while you lobby for the Intramedullary Nail? Hmmm.
Actually no. As I just spent two months in USA and saw what facilities you have over there. I think that for you applieng Ilizarov would be fun,, but here it is really just pain where the legs start....
Comments and constructive criticism is welcome,
Date: Sat, 14 Jun 2003 19:48:54 +0600
From: Alexander Chelnokov
Hello Alo,
AK> implants from Russia. I am aware that there is on the market lots of fancy Ilizarov western analogues but those are still too expencive for us. So it leaves us with limited hardware and even those that we
Is there strict control over the hospital about implant certification?
If not your department may order needed details at local factory. (Whispering - as sometimes we do).
AK> wires not perpendicular to bone and not crossing in the centre of bone etc.
The mentioned aspects are very archaic. Ideally the section of the device should be aligned to the fragment, not each separate wire. Wires/half-pins can be placed at any angle to the axis, it can be secured in any position.
AK> reassembling pretty tricky. So as I planed to nail this tibia I removed the frame
It would be nice to make x-rays without hardware.
AK> decided best treatment to be long leg cast 2-3 months
So long period of joint immobilization looks unnecessary.
AK> With my limited experience I would go for nail after 10 days of cast and if nailing fails then accurate Ilizarov again.
How do you plan to perform nailing? Do you plan to use distractor or traction table?
AK> facilities you have over there. I think that for you applying Ilizarov would be fun, but here it is really just pain where the
BTW the Ilizarov set even old included long bars with holes which allow to assembly monolateral frames which are better tolerated.
Best regards,
Date: Mon, 16 Jun 2003 01:25:08 +0530
From: DR T I GEORGE
Hi Alex,
|
The picture you showed contradicts your own statement: "Just because i'm not an expert in internal fixation techniques."
It shows that you are not just an expert but a super expert. Good work.
Date: Mon, 16 Jun 2003 07:24:34 -0500
From: Frederic B. Wilson, M.D.
Alo,
What was the rationale for waiting 2-3 months before IMN? Is there any evidence for pin tract infection? If labs are normal I would opt for limited exposure at the fracture site to obtain tissue for fresh frozen specimen. If those are normal, I would opt for IMN and bone grafting at the fracture site. You are likely to find significant fibrous tissue around the fracture site. This does not all need to be resected, but clear enough to allow more anatomic alignment. You may also need to place blocking screws A to P, lateral to the guide wire, before inserting the nail. In addition, it is not clear whether or not the fibula is united. If it is, a fibular osteotomy may need to be performed to allow realignment.
When you make your starting hole on the tibia, make sure the knee is well flexed and that you don t cheat anteriorly. Also make sure that you don t allow the reamers to progressively take more from the anterior cortex at the starting hole. I will be anxious to see the follow-up radiographs. Good luck.
Btw, I think that I would be reluctant to avoid having the necessary Ilizarov equipment simply because of the animosity towards the former Soviet Union. I know that must seem easy to say from this side of the world, but it seems that the only one who really suffers is the patient. Just a thought.
Best regards,
Date: Mon, 16 Jun 2003 08:32:02 -0400
From: James Carr
If you are worried about infection after ex-fix (and I share your concern), and unable to make the frame work as per recommendations, then I would give him a 4-6 week fixator "vacation" in a cast, followed by compression plating. He will love you for it. Bone graft based on the biology present - ie hypertrophic needs no bone graft. If in doubt, bone graft it. Except for the infection risk, nailing would handle this fracture nicely - I'll bet the last Docs started the nail too distal, thus bursting the proximal piece.
James B. Carr, MD
Palmetto Health Orthopedics
Date: Tue, 17 Jun 2003 02:05:59 +0600
From: Alexander Chelnokov
Hello All,
DTIG> Hi Alex, The picture you showed contradicts your own statement: "Just because i'm not an expert in internal fixation techniques."
Attached is an example of the "expert" level - the last case. Open lower third tibial shaft fracture, 2 weeks after injury, 30 years old male. The new fracture was revealed when the patient already has been transported from the OR. Tomorrow he is scheduled for its fixation.
It is the first such complication from about 80 tibial nailigs. What is the reason of the fracture, and what is the optimal way to fix it? I plan to apply external fixator, and 45 degree screw, and maybe 1-2 interfragmentary screw.
THX in advance.
 |
Best regards,
Date: Mon, 16 Jun 2003 20:04:46 -0400
From: Peter Trafton
Dear Alex,
I don't think I've seen such a proximal tibial fracture ? through nail entry site in many more than 80 IM nailings. How did you prepare the entry and introduce the nail? Any information that might help us avoid similar problems? Presumably no evidence of fracture there before?
I'm not sure the 45 degree screw (I assume through the nail) would do much good - too low.
I'd fix with 2 lag screws from front to back, angled proximally, one on each side of the nail, starting low enough to have thick enough bone anteriorly. I'd probably use a posteromedial plate to "neutralize", but imagine the same could be done with an ex fix.
Good luck,
Peter Trafton
Rhode Island Hospital
Date: Tue, 17 Jun 2003 18:14:24 +0530
From: DR T I GEORGE Dear Dr Alex,
All of us do have complications and each of these do teach us what could go
wrong so that we can attempt to prevent them in future. But for these
happenings how will the text books have the section on operative
complications. The "funny" thing about it is that only few are gracious
enough to admit their complication and discuss them in public.
I feel the problem could have been that the entry hole that got extended .
How do you make the opening in the entry point? Do you use an awl and find
your way with oscillating movements or do you use any instrument that needs
banging? Other possibilty is or added factor could be that a small crack
that was present during making the entry hole got extended during the nail
entry with the nail impacting on the posterior cortex. Some how I make it a
point to screen the lateral view during making the entry hole with an awl
and nail entry number of times, since even during the most confident of
times, I have seen the image betraying my confidence and found awl and nail
hitting the posterior cortex.
Having said so much, I suppose this fracture can be managed in a number of
ways. An above knee slab or a cast that immobilises the knee could get the
upper fracture to unite. An ex fix or long oblique screws or even a small
plate could be considered. I feel any of these fixations may not be adequate
to mobilse the knee confidently and hence why not just immobilisation of the
knee?
Do let us know what you have done. Best of luck.
Date: Tue, 17 Jun 2003 20:03:01 +0530 From: rajesh Why not just do a couple of interfragmentary screws percutaneously, angled
proximally from the distal fragment? Unless the frame will allow you to
mobilise the patient weight bearing, I can't see the point in going to that
extent. rajesh Date: Tue, 17 Jun 2003 22:40:28 +0600 From: Alexander Chelnokov Hello Peter, PT> nail entry site in many more than 80 IM nailings. My colleagues attended AO basic course recently reported about a half
such fractures on artificial bones used at a workshop on the technique :-) PT> How did you prepare the entry and introduce the nail? As usual by an awl. I assisted our resident, a very graceful and subtle
woman so all looked very gently and delicate. All the surgery my hands was
itching to take away the hammer and show her what is a real impact... PT> Any information that might help us avoid similar problems? Intuitively i suppose two probable reasons - too low entry hole and the
awl wasn't penetrated deep enough. PT> Presumably no evidence of fracture there before? Exactly. Except no complaints about the site before the surgery. PT> I'm not sure the 45 degree screw (I assume through the nail)
would [...] do much imagine the same could be done with an ex fix. Agree. THX for the suggestion, it supported my plan. Xrays in the next
reply. Best regards, Date: Tue, 17 Jun 2003 23:01:03 +0600 From: Alexander Chelnokov Hello Dr. George DTIG> use an awl and find your way with oscillating movements Yes. DTIG> making the entry hole got extended during the nail entry
with the nail impacting on the posterior cortex. Hmmm... I didn't think of that. The nail was inserted manually for first
10-12 cm., and only further a hammer was used. DTIG> oblique screws or even a small plate could be considered.
I feel any of these fixations may not be adequate to mobilse the knee I suppose combination of external and minimal internal fixation would
allow to mobilize the knee as well as partial WB. DTIG> Do let us know what you have done.Best of luck. I applied a simple Ilizarov frame, and after reduction inserted a locking
screw into a 45 degree hole and two AP screws "miss a nail". X-rays
attached. Best regards, Date: Wed, 18 Jun 2003 09:36:40 -0400 From: James Carr Nice bailout Alex. One cause of proximal fracture in addition to starting
too distal is extending the knee during insertion. This can lever the nail
against the femur. There are jigs to do full extension nailing with a more
lateral starting point- I have not personally used them. Date: Thu, 19 Jun 2003 22:11:13 +0600 From: Alexander Chelnokov Hello James, JC> Nice bailout Alex. One cause of proximal fracture in addition
to starting too distal is extending the knee during insertion. THX for the thought - looks likely for this case, there was a couple
of the moments... Will keep this in mind for future nailings. JC> This can lever the nail against the femur. There are jigs to
do full extension nailing with a more lateral starting point- I have Is there any Internet resources about the device? Best regards, Date: Thu, 19 Jun 2003 13:04:16 -0400 From: James Carr Alex, I believe Synthes makes that jig. Others may know more.
