Date: Tues, 7 Dec 00:05:23 +0530
Subject: Pregnant Pelvic Fx
Seeking advice on 25 y/o female s/p MVA with painful limitation ROM Rt hip. Viable fetus of 28 wk gestation. Psych hx. Normal distal neuro and vascular function.
Mark McAndrew, MD, VUMC
Date: Tue, 07 Dec 1999 22:08:27 -0600
From: Andrew H. Schmidt
Based on the single x-ray, it appears to me that your patient has an infratectal, transverse fracture of the right acetabulum. The AP roof arc appears to me to be about 45 degrees, although the quality of the x-ray was not quite good enough for me to say with confidence. In a 28 week pregnancy, I would go ahead and get Judet views to completely assess the fracture. I would not do the usual CT scan since that would involve a lot more radiation exposure to the fetus. If the roof arc is truly what I think it is on the AP view, and the Judet views are similar, then I think that the patient could be treated non-operatively. This would involve non-weight bearing for up to 12 weeks. If the patient cannot comply because of her psych history, or if the fracture displaces, then surgery could be performed. I think that the risk of surgery to the fetus at this stage would be minimal. What do your OB colleagues say?
Andrew H. Schmidt, M.D., Dept. of Orthopedic Surgery, Hennepin County Medical Center, University of Minnesota
Date: Wed, 08 Dec 1999 10:41:45 -0500
From: Mark C. Reilly, M.D.
For the most part I agree with Andrew. The fracture may be a juxtatectal transverse but the image is not clear enough to perfectly characterize the fracture from the AP alone. I would also get well-positioned Judet views and avoid the CT scan.
I am concerned, however, that on the AP, the R femoral head appears to have lost congruence with the sourcil. If the Judet views confirm this, her prognosis is poor with non-operative treatment and I would operatively reduce the fracture.
Date: Wed, 08 Dec 1999 09:18:12 -0700
From: Thomas A. DeCoster M.D.
How long post injury?
Beware of delayed fetal demise (several days after car wreck) sometimes related to abruptio placenta without regard to other treatments like ORIF acetabulum. I have done two similar patients at about 24 wks gestation. Posterior column was displaced more than 2 cm in both. ORIF with posterior column plate without radiographs (to protect the fetus). Both delivered healthy babies and both healed acetabular fractures OK and post delivery radiographs confirmed good reductions (thankfully). Plates didn't shake loose with pregnancy hormones at least in these two cases. So I think it is POSSIBLE to do successful ORIF although I don't know rates of complication.
That said, with this radiograph where the amount of displacement does not look too bad and despite painful ROM I might lean toward nonoperative treatment of this acetabular fracture.
T DeCoster
Date: Wed, 8 Dec 1999 23:25:17 +0200
From: Nachshon Shazar
I would like to present an acetabular fx in which the AP view showed even less displacement, but Judet view proved it to be a 6 mm displaced posterior column acetabular fx. (X ray attached) I believe that the case we are discussing is a displaced posterior column fx (iliac view is needed) and ORIF is probably indicated.

| 
|  |
Nachshon Shazar, Tel Aviv, Israel
Date: Thu, 9 Dec 1999 21:37:24 -0800 (PST)
From: Chip Routt
hi mark-
when was her injury?
maybe more data is necessary to accurately classify and treat...2 Judets and perhaps some selective axial CT images based on the Judet findings would be very helpful.
her hip is not congruent...need more info.
happy holidays - chip
From: Mark McAndrew
Date: Sun, 12 Dec 1999 16:04:40 -0600
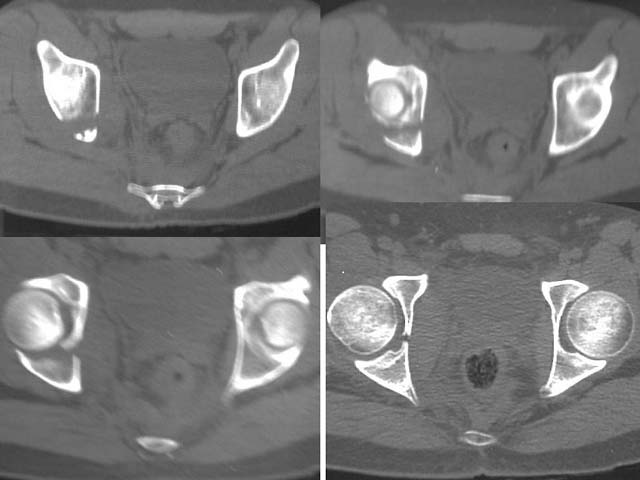
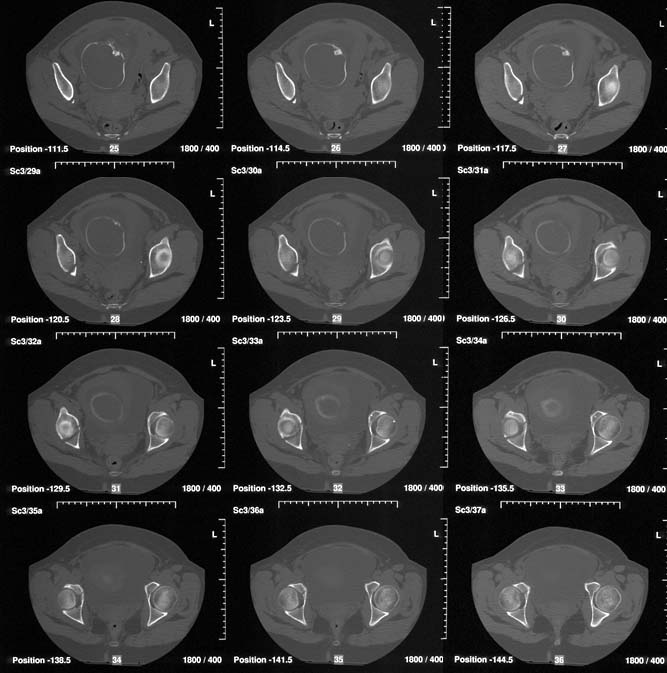
The CT showed a max displacement of 5 mm. Iliac and obturator views are obtained.

| 
|  |
 |
Mark McAndrew, MD, VUMC
Date: Tues, 14 Dec 1999 12:00
From: Bill Burman
Radiation Relative Values (.001 Gray = 1 mGy = .1 rad = .1 mSv)
3/69 abstracts returned from NLM Grateful Med using the search terms "third trimester" and "radiation".
Date: Thu, 16 Dec 1999 18:00:37 -0700
From: Thomas A. DeCoster M.D.
After reviewing the Judet obliques and CT, I would tend toward nonoperative treatment. The maximum displacement is on the iliac oblique and the joint is certainly not perfectly congruent. However the femoral head seems nicely aligned to the acetabulum on all cuts of the CT and plain films.
Risk/benefit analysis would include assessment of the expected outcome with nonoperative treatment, the expected outcome with operative treatment (the difference being the benefit), the direct risks of operative treatment (infection etc.) plus the indirect risks (fetal demise, childhood cancer etc).
Date: Thu, 16 Dec 1999 20:54:23 -0800
From: Steve Olson, MD
Mark:
I looked at the AP pelvis, Judet views, and CT you provided. This patient appears to meet all roof-arc criteria, and all ct-arc criteria (by my eval ~9 mm below vertex). The only question is late instability. I would follow the protocol of Tornetta et al for stress view under flouro (JBJS-BR 1999 January journal). If the femoral head stays congruent with the superior acetabular articular surface then non-operative management. (I think it will).
Good Luck, Happy Holidays