



Date: Sat, 9 Mar 2002 15:01:12 EST
Subject: Posteromedial Tibial Plateau Fx Approach
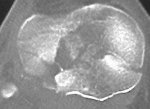
Displaced posteromedial tibial plateau fracture in 44 year old female (fell down stairs). AP alignment is OK Lateral tibial plateau is OK.
Large displaced posteromedial fragment seen on lateral view and 3+ lachman because of tibial spine avulsion by ACL.
What is the surgical approach?
(1) 1 long median parapatellar arthrotomy to secure ACL tibial spine and strip MCL and pes to get to the posteromedial tibial plateau fragment
or
(2) smaller anterior and posteromedial incisions.
Does an incision posterior to the MCL and anterior to the hamstrings give enough visualization of the posterior medial plateau?
Does the LISS plate work well in this situation on the medial side?
Thank you.
Mike Messieh
Date: Sat, 23 Mar 2002 20:13:46 EST
From: Tadabq
I have used the 2 incision approach you mentioned in this situation with a posteromedial incision. It was described in JOT a few years ago. A regular plate works fine if you get all the way to the apex of that posterior medial fragment, which is otherwise very difficult to impossible to do, even with an extensive subcapsular dissection from the front.
Tom DeCoster
Date: Sat, 23 Mar 2002 19:21:29 -0600
From: Adam Starr
This may be crazy, but I approach these using a long midline exposure. I do a medial parapatellar arthrotomy and lift the soft tissues off the medial plateau, all the way 'round back.
A longer midline incision prevents undue tension on the skin.
I find I can see the medial plateau much better. It's easier for me to reach the spike at the bottom of the fracture, and easier to judge the reduction at the joint.
It's a fun exposure.
It goes without saying (I hope) that the skin has to be in good shape before you can do it this way.
I have never enjoyed the posteromedial exposure. I hate dancing around the pes tendons.
Date: Sun, 24 Mar 2002 11:00 AM
From: Bill Burman
Mike
While waiting for the debate to develop on this topic, you might consider the following:
>Does an incision posterior to the MCL and anterior to the hamstrings give enough visualization of the posterior medial plateau?
Apparently the Hannover group says yes.
Unfallchirurg 1997 Dec;100(12):957-67
They also say "Surgical exposure of these fractures from anterior requires major soft tissue dissection and has a significant complication rate."
Georgiadis says go posterior to the hamstrings.
J Bone Joint Surg Br 1994 Mar;76(2):285-9
>Does the LISS plate work well in this situation on the medial side?
Closest reference I could find:
DuWayne A. Carlson, Percutaneous Plating of Tibial Plafond and Plateau Fractures: Preliminary Report
Overview Refs:
Date: Sun, 24 Mar 2002 11:25:03 EST
From: MMessieh
From the discussion so far, it appears that the posteromedial incision is helpful. However, there may be some disadvantages:
1. There is no visualization of the medial tibial plateau.
2. The butress plate may help prevent inferior displacement but poor resistance against flexion or varus of the medial plateau.
3. ACL tears and intercondylar eminence fractures cannot be adressed through this approach.
4. If combined with the anterior lateral approach, the eventual total knee incision will be between these 2 incisions.
Regarding LISS plating for type 4 fractures, it occurred to me that an up to date web based list of implants/devices by anatomical areas would be very useful. The surgeon would see all of the device options available and make the most reasonable choice for the case. Just as CT scans have been shown to alter treatment at times, a list of available implants by anatomical areas could alter treatment as well, I think.
mike
Date: Sun, 24 Mar 2002 16:07:22 EST
From: HPLobenhof
hello,
I am the author of the German paper on a posteromedial approach to this fracture published in Unfallchirurg 1997. A description and an X-ray is also published in CORR 292, p. 97-100, fig. 6a-c. This posteromedial approach works well and allows you to see the spike of the fragment. You can apply an anti-glide plate over the spike of the fragment and supplementary transverse lag screws which avoid varus deviation of the fragment. LISS plate is too big for this purpose. You could use a small fragment LC-LCP reconstruction plate but this is not necessary in my experience. The case in CORR is exactly the one you discuss. The hamstrings usually need only to be retracted, in some cases with a long spike they can be incised and sutured at the end of the procedure. I would use a posteromedial incision and a small anterior incision for the tibial eminence.
The alternative for me would be to start in prone position, use a posterior incision, retract the medial gastro and the popliteus, perform direct fixation and then turn the patient with the draping and fix the tibial spine back. This is also a good option.
Philipp Lobenhoffer
Hannover
Date: Mon, 25 Mar 2002 14:10:30 -0500
From: James Carr
I have approached these with a small anterolateral incision, and a posteromedial incision. The anterolateral one lets you get at the ACL, and also facilitates cleaning debris from lat-med plateaus. The anterolateral one is just at the margin of the patellar tendon, and doesn't have to go more proximal than the distal 1/3 of the patella. Many times the spine piece can be fixed with a screw. The postero medial lifts the pes anteriorly, then reduces the plateau indirectly by extraarticular landmarks. In rare instances, posterior capsulotomies can be performed. The plate is put right on top of the MCL- no subperiosteal stripping required. I haven't used the LISS, but have handled a number of late posteromedial subluxations when the surgeon didn't buttress that side.
To address a few concerns - The posteromedial approach can be a major pain in the butt. Sometimes a small roll under the opposite hip will help. It is not intended to visualize the joint. The anterolateral approach I describe can easily be extended into a total knee approach.
Jim Carr
Date: Mon, 25 Mar 2002 18:16:09 -0700
From: Kanlic, Enes M., M.D.
These posteromedial and posterolateral approaches are often the only applicable solutions. I have used them in many cases, mostly as separate incisions, or occasionaly getting to the pathology through anterior skin and fascia incision, bending the knee and approaching posterior fracture behind MCL and/or LCL.
|
|
|
|
|
Here is the attached example of medial and lateral posterior tibial plateau fracture approached through mentioned posterior M and L incisions.
 |
 |
Sincerely,
Enes M. Kanlic, M.D., Ph.D.
Associate Professor
Texas Tech University HSC
Orthopaedic Surgery Dept.
El Paso, Texas 79905