


Date: Wed, 9 Apr 2003 17:58:57 -0400
Subject: Floating Knee - Proximal Tibial Nonunion
Question for the transport gurus
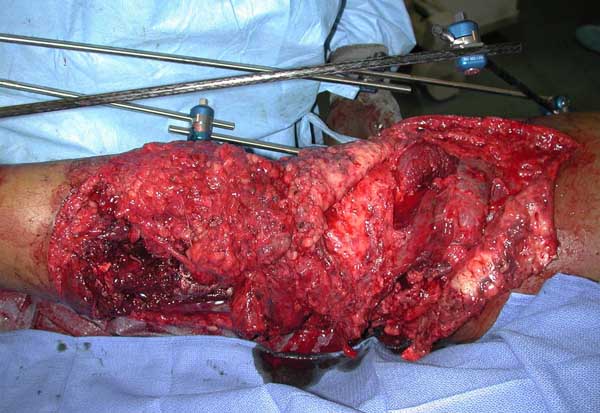
Briefly 22 yo male rollover MVA 1 yr ago. Isolated lower extremity injury. 3b open distal 1/3 femur and proximal 1/3 tib/fib (ipsilateral). Lots of debris dirt grass clothes and carpet. Treated emergently with debridement and spanning frame.
|
|
|
 |
 |
Flaped within week. Frame removed and converted to nails (retro femur) prior to flap. Had proximal tibial defect after initial debridement. Soft tissue envelope healed.
 |
 |
 |
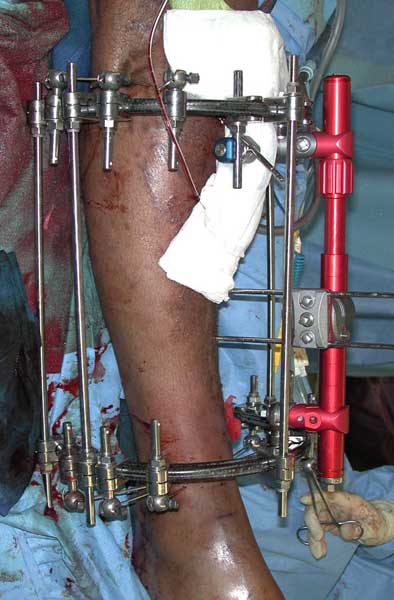
Bone grafted proximal tibial defect @ 8-10 wks. Graft resorbed. Noted to develop drainage from distal ex fix pin site approx 6 mo post injury. MSSA pan sensitive. Local wound care and Keflex initiated. Returned to OR for removal of nail, debridement of pinsite, reaming canal , resection of nonunion site and application of fine wire frame for transport.
 |
 |
|
Placed on 6 wk course IV Ancef. (same pan sensitive bug at debridement). CRP, ESR normalized. Presently off abx. with no clinical signs of infection other than he's not making regenerate. I've halted transport and waited 4 wks with no real change. Any suggestions when not seeing regenerate. Any suggestions on stimulating regenerate? Thanks in advance for the input.
Jason Nascone
Washington DC
Date: Thu, 10 Apr 2003 12:23:18 EDT
From: Tadabq
Regarding case of poor regenerate during bone transport for segmental defect of the proximal tibial metaphysis.
I would consider continuing the transport. The regenerate will often begin to show up. Also external electrical stimulation (or presumably other stimulants like ultrasound) can be helpful. Li, Simpson and Kenwright have shown injectable BMP enhances regenerate in rabbits (JOR 2000) but I might reserve that to completion of docking and combining with autogenous bone grafting of both sites.
You might also review your techniques to make sure you are doing everything optimally. Technique of corticotomy, stabilty of the frame, rate and rhythm of distraction, patient nutrition, smoking? all play a role in reliable regenerate formation.
TD
Date: Sun, 13 Apr 2003 23:14:41 +0600
From: Alexander Chelnokov
Hello Jason,
JN> defect @ 8-10 wks. Graft resorbed. Noted to develop drainage from distal ex fix pin site approx 6 mo post injury. MSSA pan sensitive. Local wound care and Keflex initiated. Returned to OR for removal of nail, debridement of pinsite, reaming canal , resection of nonunion site and application of fine wire frame for transport.
Where the infected pin site was located? How does the wound after its debridement relate to the corticotomy site? The photo with ex-fix doesn't show either. How was corticotomy of the distal tibia performed? I expected to see 0.5 cm wound on the anterior surface of the tibia - but didn't find it. What instrument and technique were used for bone section?
JN> Any suggestions when not seeing regenerate.
Poor regenerate response most likely could be due to bone end devitalization by traumatic corticotomy and/or periosteal stripping. Other obvious reasons are inappropriate speed of transport and its early start.
JN>Any suggestions on stimulating regenerate?
There are a lot of tricks with the fixator, AFAIK practice (not evidence) based. One may decrease the gap partially or even to pre-distraction level, wait 2-3 weeks then start distraction again, with lesser temp - 0.5 mm/day. Or maybe continue distraction as is after the pause with temp 0.25 - 0.5 mm daily. As a reserve keep in mind reduction of the failed site, with another, more proximal, closed corticotomy performed as delicate as possible. Since details about the technique and other related matter were not presented hardly ever more definitive advice can be given. Good luck and pls keep us informed.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 14 Apr 2003 11:36:00 -0400
From: Jason Nascone
Alex
The pin site was just proximal to the distal corticotomy. Corticotomy performed via ant medial incision, 3.2 drill, osteotome and osteoclasis using the ring. The pin site IS close to the corticotomy site and this is one of my concerns given the infection. The soft tissues were respected. Do you think the nail/ reaming play a role as well?
Jason Nascone
Date: Mon, 14 Apr 2003 23:52:05 +0600
From: Alexander Chelnokov
Hello Jason,
JN> The pin site was just proximal to the distal corticotomy. Corticotomy performed via ant medial incision, 3.2 drill, osteotome and osteoclasis using the ring.
Colleagues of mine who daily do limb lengthening procedures strictly recommend to use only small (5 mm) chisel through a stab wound. No drills, no oscillating saws etc. Too expressive osteoclasis can produce even full diameter displacement or lack of contact prior to transport which also leads to weak regenerate. I don't insist that's the reason, just try to exclude anything which is not impossible.
JN> The pin site IS close to the corticotomy site and this is one of my concerns given the infection.
Of course active infection (pus) in the zone of distraction prevents any new bone formation. But the report doesn't support that the situation goes this way.
JN> The soft tissues were respected. Do you think the nail/ reaming play a role as well?
Many examples of lengthening over the nail demonstrate that the role is far from fatal though full preservation of the canal + viable periosteal tissues provide best possible regenerate.
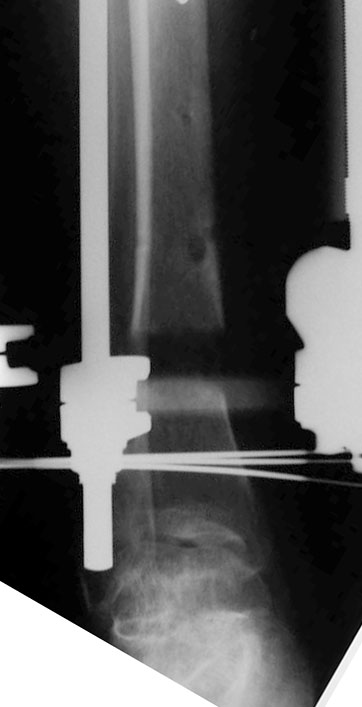
I tried to tune images and something is visible in the gap after some enlightment. Can you pls re-do xrays (maybe only of the zone) to provide more soft image?
Do you plan conversion to the locked IM nail after transport?
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Wed, 16 Apr 2003 09:22:00 -0400
From: Jason Nascone
Alex
Here is a close up of the regenerate under hot light. There is a small
amount of wispy regenerate. Would you continue advancing? Ive placed a bone
stim over the regen site. Most likey will convert to nail.
 |
Thanks
Jason
Date: Thu, 17 Apr 2003 00:22:06 +0600
From: Alexander Chelnokov
Hello Jason,
JN> Here is a close up of the regenerate under hot light. There is a small amount of wispy regenerate. Would you continue advancing?
Expected time of maturation looks too long so in case of ex-fix as definitive stabilization i would prefer to drop distraction back and re-do corticotomy higher, at the middle of the segmental fragment.
JN> Ive placed a bone stim over the regen site. Most likey will convert to nail.
It seems to me there is high risk to go to the situation you started from, just with the gap located at another place. Intuitively, probability to have the defect healed before the nail gets broken looks less than acceptable. Maybe thick nail with thick screws would resist long enough. Also bone grafting of the distal defect can be presumed in case of poor bone formation revealed in 3-4 months after conversion.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia