


Date: Tue, 11 Dec 2001 22:47:30 -0000
From: Nuno Craveiro Lopes
Subject: Perthes Disease ??
Dear all,
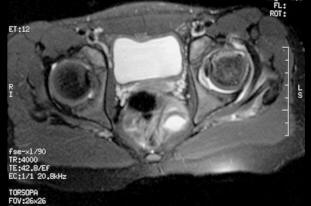
I appreciate some advise on this case. 11 y o girl doing high performance gymnastics in USA. On a fall over the left foot have done a forced medial rotation of the left hip, feeling pain on the buttock and thigh. Stopped the activity for a week and returning to sport, didn't reach the same performance, complaining of pain and limping when she make efforts, this lead her to abandon gymnastics. It have been diagnosed as Perthes disease. I am attaching xr and relevant mri. Your opinion is welcomed.
|
|
|
|
|
Best regards,
Date: Wed, 12 Dec 2001 06:15:25 -0600
From: Adam Starr
Hi Dr. Lopes.
Those images look a lot like perthes disease to me.
There was a paper in JBJS Am some years ago where the authors found that many (maybe all - I can't remember exactly) patients with Perthes had low serum levels of protein C and protein S.
If there's a question about the diagnosis, maybe you could check those tests and see if the levels ARE low. If low, then that would make me consider perthes even more strongly.
If it IS perthes, then her relatively advanced age at presentation hurts her - and even worse, as a girl, she has even less time for her femoral head to remodel.
But, her femoral head is still spherical, it looks to be about the same size as the other head, and her joint space is preserved. Those are all good things.
I'm not a pediatric orthopaedic surgeon. I think this is perthes disease, but I'd send her to a center where they see a lot of perthes to be sure.
The history of a fall during gymnastics may be a red herring. Kids fall all the time, especially in gymnastics. I wonder if that fall really led to this problem?
Adam Starr
Dallas, Texas
Date: Wed, 12 Dec 2001 08:18:30 -0500
From: Bill Burman
There was a paper in JBJS Am some years ago where the authors found that many (maybe all - I can't remember exactly) patients with Perthes had low serum levels of protein C and protein S.
As usual, the literature appears to be muddled on this:
Glueck CJ, Crawford A, Roy D, Freiberg R, Glueck H, Stroop D.,Association of antithrombotic factor deficiencies and hypofibrinolysis with Legg-Perthes disease.,J Bone Joint Surg Am. 1996 Jan;78(1):3-13.
"Thirty-three (75 per cent) of forty-four unselected children who had Legg-Perthes disease were found to have coagulation abnormalities. Twenty-three children had thrombophilia (a deficiency in antithrombotic factor C or S, with an increased tendency toward thrombosis); nineteen of the twenty-three children had protein-C deficiency and four had protein-S deficiency."
----------------------
Kealey WD, Mayne EE, McDonald W, Murray P, Cosgrove AP., The role of coagulation abnormalities in the development of Perthes' disease. J Bone Joint Surg Br. 2000 Jul;82(5):744-6.
"We reviewed 139 children with Perthes' disease and compared them with a control group of 220 aged- and gender-matched healthy primary schoolchildren with similar racial and ethnic backgrounds. There were no significant deficiencies of antithrombotic factors protein C, protein S, antithrombin III or resistance to activated protein C."
Date: Wed, 12 Dec 2001 12:37:58 -0500
From: Benedetti Gary E Maj
I reviewed this case with our Pediatric Orthopaedic Surgeon (Jeff Mikutis):
"Looks like Perthes Dx. Injury most likely unrelated. Perthes can present in children 2 to 13 yo and in an 11 yo, the prognosis is worse. This child will probably need an osteotomy(ies) for containment. Would do routine labwork, i.e. CBC and ESR, first though to rule out other causes. Jeff"
Best regards,
Gary E. Benedetti, MAJ, USAF, MC, FS
Orthopaedic Trauma Surgery
Date: Wed, 12 Dec 2001 20:36:37 -0500
From: JOHN ROBERTS
The eleven year old female gymnast presents with an xray image of the left hip which looks more benign than the MRI which shows coxa plana with resorption of bone in a large area of the femoral capital epiphysis and widening of the femoral neck. These changes and the patient's gender and age mean a poor prognosis for Legg-Perthes disease which I believe this case represents. Was the MRI done somewhat later in the course of time than the X-rays? I could not make out dates on the images. There is one feature of the MRI which might be favorable: the enlarging femoral head does not seem to extrude far beyond the edge of the acetabulum as marked by the thorn sign. This indicates that satisfactory containment might still be obtained by upper femoral varus-producing osteotomy. I would confirm this possiblity by a dynamic arthrogram at the time of surgery; if the femoral head centers well enough with up to 30 degrees abduction for the edge of the acetabulum to drop down around it, the upper femoral osteotomy might bring a good short term outcome. Otherwise, I might consider a double osteomy: upper femoral and innominate. Left alone, the hip will probably go on to hinge-abduction with attendant pain and stiffness.
Dear All,
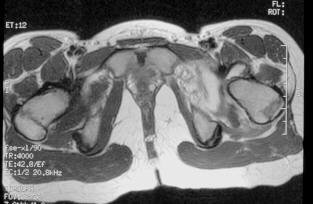
Regarding this case, I am grateful by your opinion. After careful analysis of the history and films, I am convinced that this is not a Perthes disease. In fact, on this case there are a violent traumatic event that have provoked the lesion, which is not compatible with Perthes. On the other hand, the MRI pattern is not what I am used to seeing. The patient presents a voluminous joint effusion and a image of anterior impaction of the femoral head with a thin layer of subchondral necrosis under the compacted zone (jb02).
 |
 |
As we interpret this patient's lesion, it is not Perthes nor traumatic AVN; it is a crush injury of the head with sub-chondral fracture and necrosis of the underlying bone tissue by impaction. The probable mechanism can be explained by the immature bone structure subjected to intense training. The young lady was doing an exercise that only a few athletes do - triple spinning, rotating the body anticlockwise and landing unbalanced over the left foot. Inertia violently medially rotated the limb, firstly stretching the lateral rotator muscles to its limit, then doing a impaction fracture of the anterior head on the anterior wall of the acetabulum, and finally, instead of a dislocation, muscular/tendinous rupture happens at the rotator muscles. We have proposed to complete the image study with a US scan and MRI on T1 sequence and sagittal plane. If we can confirm this type of lesion, we intend to do a transphyseal neck-head tunneling, dis-impaction of the head and bone graft thru the tunneling. The patient came this week from USA to be studied and treated on our hospital. I hope to be able to show you the new images next Monday.
Best regards,
Date: Tue, 18 Dec 2001 15:07:06 -0000
From: Nuno Craveiro Lopes
Dear All,
We have completed the study of this patient which confirmed the diagnosis. She have been operated by the described procedure, which can be seen on:
http://clientes.netvisao.pt/nfrancac/case04.htm
We intend to keep the patient without weight bearing for a month and protected with a abduction-flection brace until we can see signs of consolidation. Has anybody references of similar cases ?
Best regards,