

Date: Wed, 23 Jan 2002 13:56:16 -0500
Subject: Femoral Neck Nonunion
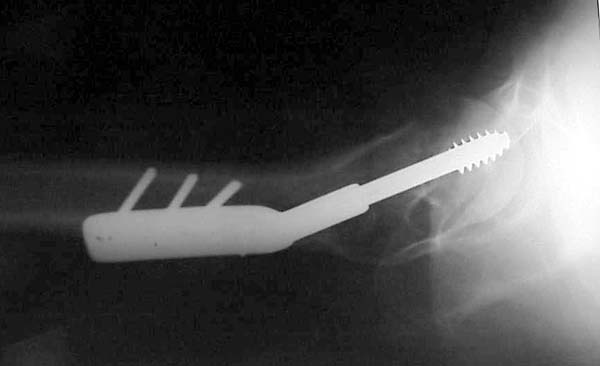
Thisis a 37 yo male that was in Domincan Republic 10 months ago visiting his mother when he had a MC accident. He apparently had a displaced FN fx stabilized w/a SHS that lost fixation and was revised at 1 month.
|
|
|
I have no previous xrays. He was unable to travel due to pain until recently when he presented this week. He has not been ambulatory since his injury and c/o daily significant pain. He has never had any problems w/ his wound and is otherwise healthy and previously worked as a professional dancer. He has minmal motion at hip due to pain inhibition. ESR 35. Joint aspiration pending.
Would anyone consider a valgus osteotomy and blade plate or is this too unlikely to succeed? The other option is a THA if no evidence of infection is found.
Thanks
Bill Obremskey MD MPH
University of North Carolina
Dept. of Orthopedics
Date: Wed, 23 Jan 2002 15:01:13 -0600
From: Anglen, Jeffrey
I think valgus osteotomy will be successful. Careful planning is necessary for fixation.
Jeffrey O. Anglen, MD FACS
Associate Professor of Orthopaedics
Chief, Orthopaedic Trauma Service
Columbia, MO
Date: Wed, 23 Jan 2002 17:10:54 -0600
From: Wasylenko, Mark
He has a nonunion of a femoral neck fracture. Is the head avascular? Get an MRI. If the head is dead, osteotomy will not help, and he might as well have a total hip.
Mark Wasylenko MD
Date: Thurs, 24 Jan 2002 7:38 AM
From: Bill Burman
>If the head is dead, osteotomy will not help
It appears that the OTA Fracture Conference presentation on femoral neck nonunion would argue that femoral head avascular necrosis is not necessarily a contraindication to valgus osteotomy. See
Ed Harvey, (ex Urbaniak fellow), would such a case be accepted by the Duke fibula transplant team?
i.e. Urbaniak JR, Coogan PG, Gunneson EB, Nunley JA; Treatment of osteonecrosis of the femoral head with free vascularized fibular grafting. A long-term follow-up study of one hundred and three hips.; J Bone Joint Surg Am 1995 May;77(5):681-94
Bill Burman, MD
HWB Foundation
Date: Thu, 24 Jan 2002 22:12:11 +0500
From: Alexander Chelnokov
BB> It appears that the OTA Fracture Conference presentation on femoral neck nonunion would argue that femoral head avascular necrosis is not necessarily a contraindication to valgus osteotomy.
Exactly. Also - why only valgus? Why not perform medialization to overlap the gap? Of course it results with difficulties if THA would be required later. But it provides painless and functional limb even without full neck union and with necrosis. Overloading of knee medial compartment doesn't seem to be a big trouble.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Thurs, 24 Jan 2002 1:25 PM
From: Bill Burman
Medialization of the head-neck segment or lateralization of the femoral shaft is also covered by the OTA Fracture Conference presentation on femoral neck nonunion.
Bill Burman, MD
HWB Foundation
Date: Thu, 24 Jan 2002 21:53:34 -0500
From: edward harvey
If the head is dead, osteotomy will not help
I agree that if the head is 100% dead then there is little chance of saving the head.
Some people think differently ( Orthopedics 1999 May;22(5):493-9 Vascularized iliac bone graft for displaced femoral neck fractures in young adults. Chang MC, Lo WH, Chen TH.)
Dr Urbaniak has an unpublished experience (perhaps presented at AAOS 2 years ago) of at least 19 femoral neck nonunions treated with fibular graft. They all did pretty well as near as I can remember and there were some younger patients that had large head involvement. At this patient's age I probably would only opt for that if he had near normal flow to the head.
I think a bigger concern here is infection. Actually the Pauwels angle is not totally vertical and with solid dynamic fixation of any kind done adequately it should have healed. Posterior comminution might have caught up with it though. Personally, I have found in displaced cases or those with comminution or shortening that a valgus osteotomy with a posterior bone pedicle works well. I think the Toronto group has a small series of these with good results (not published yet)
It appears that the OTA Fracture Conference presentation on femoral neck nonunion would argue that femoral head avascular necrosis is not necessarily a contraindication to valgus osteotomy.
I think it would definitely depend on a lot of factors including size of head involvement, step in femoral head, location of lesion, BMI, other comorbidities etc. etc.
Edward J Harvey MDCM FRCSC
Hand and Microvascular / Trauma
Medical Director: Fracture/Bone Metabolism
McGill University -MUHC
Montreal Qc