

Date: Tue, 07 May 2002 06:29:49 -0400
Subject: Severe Pilon
This is a 60 yo healthy construction worker who fell 12 feet and sustained bilateral pilons, left 41C3 prox tibia fx, and right distal radius fx. All fxs were closed and initially ex fixed. The right pilon is severe and I am not sure that the articular surface is reconstructable.
He has bilateral fx blisters and maybe some full thickness necrosis laterally over the fibula on the right. I have never considered primary fusion w/ a pilon, but this is an option I am considering after his soft tissues are healed. Anyone have any experience or thoughts.�
|
|
 |
 |
 |
 |
Bill Obremskey
UNC Dept of Orthopedics
Date: Tue, 07 May 2002 12:22:14 -0400
From: James Carr
I agree totally with your rx to date. I would try to get him to osseous union in the frame, and then see what he needs. He may need nothing further. Primary fusion can be done, and would require some type of long plate e.g. blade. I have a few pilons over the years that I have treated with ex-fix followed by later reconstruction. A few go on to spontaneous ankle fusion, or painless ankylosis. I have done total ankles on three, and they have done well. Another with bilaterals didn't need anything on one side (functional ankle fusion), and the other side needed a fusion due to infection from poorly conceived ORIF. One problem that does arise is nonunion of the shaft to the joint fragments. His talus appears centered nicely under the tibia, and this is key. If it appears that he needs something further done, I would remove the fixator in the OR, and really clean out the pin sites. Watch the full thickness contusions closely, and hopefully that will heal with observation.
Jim Carr
Date: Tue, 07 May 2002 14:50:49 -0400
From: J. Tracy Watson
Primary fusion in the face of this degree of comminution is extremely (impossible) difficult to achieve without a major cluster....this usually requires resection of the comminution followed by bone transport ....which,,,, having been there, I wouldn't recommend to anyone I call my friend....rather...........I would span the fractures and let them heal as much as possible to reconstruct bone stock for a later fusion....do you have a post distraction CT scan...sometimes you can joy stick fragments into better position and cannulated screw them is possible....however with these significant smash ups....take the minimalist approach ......you might also be surprised to find that even though the x-ray looks horrible their function may be better....to the extent you can delay a fusion for some months
JTW
Date: Thu, 9 May 2002 19:51:04 +0100
From: Nuno Craveiro Lopes
Dear William,
I recommend ligamentotaxis and minimal osteosyntesis for this case as on the attached file.
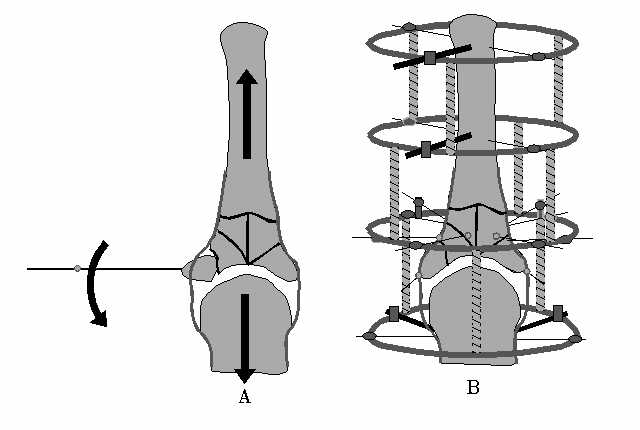 |
If later arthrodesis is necessary, it will be possible to do it easily because there are no hardware in place.
Best regards,
Nuno Craveiro Lopes
Almada, Portugal
http://clientes.netvisao.pt/nfrancac/
Date: Sun, 12 May 2002 11:01:18 +0600
From: Alexander Chelnokov
Hello William,
WO> is severe and I am not sure that the articular surface is reconstructable. He has bilateral fx blisters and maybe some full thickness necrosis laterally over the fibula on the right. I have never considered primary fusion w/ a pilon, but this is an option
I would postpone the idea of fusion. There is a chance to improve position of fragments at least to provide better bone stock for later fusion. I would use ring at the distal level (at your side even a radiolucent one must be available) and some olive half-wires to push together main fragments of the pilon under fluoroscopic control to keep them inside their anatomic contour. After best possible reduction the pilon should be fixed with 4-5 olive crossing wires and alignment with the shaft performed. Then i would remove wires/pins from the foot to allow early ankle ROM. I remember some cases where fusion was not performed at least within 2-3 years after the injury, especially if patient was a tourist/alpinist - they are crazy and continue jumping/climbing.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str. Bankovsky, 7. Ekaterinburg 620014 Russia