

Date: Thu, 30 Oct 2003 06:21:21 -0600
Subject: Proximal Humerus Fx
From: Obremskey, William T
49 yo male RHD architect 3 mos s/p left prox humerus fx/dislocation in MCA presented today wanting know if he had any other treatment options at this time. He had initial PP, which was better reduced, but fell back into valgus impaction. He has 45 degrees FF, 40 degrees Abduction, 20 degrees ER of motion now w/ limited function.
Anyone consider ORIF and use Norian as reported for acute valgus impacted fx in Sept JBJS, Hemiarthroplasty or leave it alone?
|
|
William T Obremskey MD MPH
Vanderbilt University
Orthopedic Trauma Division
Nashville, TN 37232-3450
Bill Obremskey
Date: Thu, 30 Oct 2003 08:33:39 EST
From: Aobonedoc
Hello:
I assume MCA is MVA representing high energy injury.
The inferior subluxation appearance on the AP could represent a subtle plexus injury so one should give this some thought. A neuropraxic injury, especially mild can be difficult to diagnose on the first eval and with a fraxture. My last humerus shaft fx from a motorcyle accident had a plexus injury that I did not big up the first time around. It appears the fracture has not healed yet on the xray. I would not operate yet at three months. I would wait. I have used OP-1 twice (the Stryker BMP, $5,0000) twice and have found it to work quickly. If surgery opted for, Synthes has a nail with a spiral blade type proximal fixation, I have never use. I think a hemi most likey would be needeed He might be able to live with a nondominate bad shoulder given his job. In Cook county here (with lawyers everywhere) I would move slowly and get to now him. He may do poorly with anything. In seven years here I have not had a nonunion or needed to do a hemi for a fracture in a young person. Good luck.
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005
Date: Thu, 30 Oct 2003 13:08:59 -0600
From: Obremskey, William T
Thanks. MCA is mororcycle accident. I am sure he had a slight neurologic injury as he had an inferior dislocation (subluxio erectae) He nicely describes his arm stuck up over his head. He states his axillary sensation is normal now.
Bill
Date: Thu, 30 Oct 2003 09:22:00 -0600
From: Anglen, Jeffrey
My vote is hemiarthroplasty if it is painful, nothing if it is not. I would not be optimistic about improving motion.
Jeff
Jeffrey O. Anglen MD FACS
Boone Orthopaedic Associates
Clinical Professor of Orthopaedics
University of Missouri
Date: Thu, 30 Oct 2003 10:56:37 -0600
From: Frederic B. Wilson, M.D.
Bill,
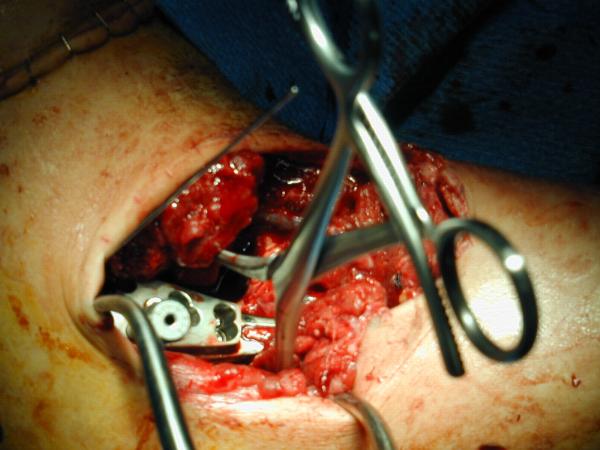
I would consider using the Synthes Proximal Humerus Locking Plate through a deltopectoral incision. After disimpacting the head you should be able to get good stabilization even in this very osteoporotic bone with the combination of converging and diverging holes. I would fill in the resulting defect with your bone volume replacement of choice. We still tend to favor autologous bone graft but have also used Norian (the semisolid putty rather than the runny liquid) and other bone graft substitutes. I will try to dig up some intraoperative and clinical photos as well as radiographs.
The attached photos show a bit of the technique.
 |
 |
 |
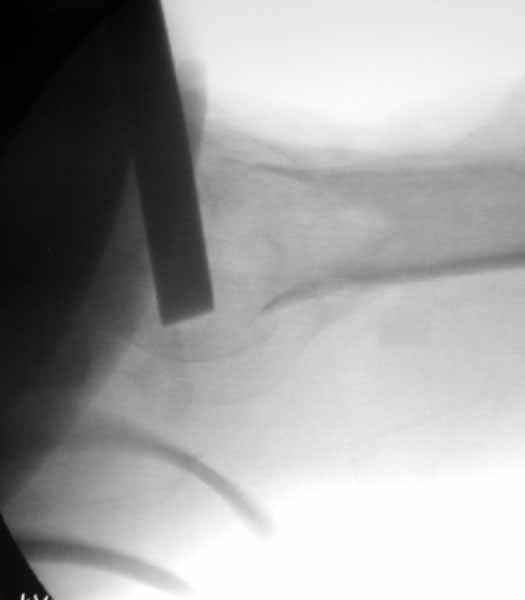
This was a 23 yo male run over by a boat with multiple propeller injuries. The fixation was carried out after several washouts with good granulation beginning and no evidence of infection. We utilized the one of the lacerations for our modified deltopectoral approach as shown in the first photo. The second photo shows the plate in place, held with a tenaculum forceps. The K-wire fits through the most superior hole in the plate with it's attached template guide. It should skim just superior to the tuberosities across the superior head and is only for positioning the plate. The third photo shows an intraoperative fluoro shot of the plate in position. The K-wire looks to be a little inferior but it may be projection. We have placed a screw through a slotted hole on the shaft to allow proximal and distal correction while maintaining rotational alignment. You can see the drill bit through the tower in one of the proximal locking holes. Sorry these aren't the greatest. I will try to dig up some better shots and some x-rays. I echo the sentiments of others that he is not likely to gain a tremendous amount of motion but we have been surprised on several occasions. From the radiographs you provided it appears that the tuberosities and, therefore, probably the rotator cuff attachments are in the ballpark although you may find it necessary to tack those down with sutures through the plate to restore the integrity of the cuff. Be prepared for the subluxation to persist for quite a while even with stabilization but it will likely improve with therapy if the cuff is attached. I have started these patients on passive, patient controlled ROM on POD #1 with flexion to 90 degrees, abduction to 70-90 degrees, and internal and external rotation to 90 degrees and neutral respectively. I'm encouraged that some recent articles have looked at comparisons between ORIF and hemiarthroplasty for Neer IIIs and IV and shown very similar results. I will send the references as soon as I am able to locate the article in my mountain of journal club articles waiting to be filed. We don't have a large series yet because the plates are relatively new (I think we were a test market) but in the dozen or so we have done we have not had any nonunions and all have had significant improvement in pain. Good luck. Warmest regards,
Frederic B. Wilson, M.D.
Trauma & Adult Reconstruction
ETMC First Physicians
Tyler, TX, 7570
Date: 10/30/03 01:03PM
From: william.obremskey
Fred,
Thanks for the info. I use the plate frequently, but never in this type of nonunion w/ a thin piece of humeral head. My concern is maintaining fixation in the head w/ the gap that will be present after repositioning. Thanks for the pics.
Bill
Date: Thu, 30 Oct 2003 17:38:07 -0600
From: Frederic B. Wilson, M.D.
Bill,
It's hard to tell from the xrays exactly how thin the head fragment is but I wonder if you were able to get screws right up to the subchondral bone, backfilling the impacted area well with bone graft, and be a little more protective, if you wouldn't be able to get it to heal. I think that a hemiarthroplasty, while certainly a reasonable choice, burns another bridge. Tough case for sure.
Fred
Date: Thu, 30 Oct 2003 14:39:34 -0600
From: Steven Rabin
I'd replace it at this point. But if you decide to fix it, i'd use the fixed angled locked screw proximal humerus plate because I think it gives opportunity for many fixed angled points of fixation...more than the single blade for the rod. an example attached (although admittedly not for a nonunion).
 |
 |
steve rabin
Date: Wed, 12 Nov 2003 17:28:01 -0600
From: Obremskey, William T
Attached are pics of malunion w/ osteotomy and fixation w/ Norian in gap after improving valgus impaction.
Xrays look better. We will see if he improves as well.
 |
 |
 |
 |
Bill
William T Obremskey MD MPH
Vanderbilt University
Orthopedic Trauma Division
Nashville, TN 37232-3450