



Date: Sun, 25 Jun 2000 20:00:28 -0500
Subject: Smashed Talus fracture
From: Rodrigo Pesantez
Dear all,
This is a 16 years old girl who felt down from a 6th floor. She sustained a Tscherne O3 Talus Fracture, no other injuries (spine, pelvis, etc. are OK), I did and I&D and an spanning x-fix, plastic surgery did a flap and now she is 2 weeks out of her injury. Any suggestions for her definitive management?
|
|
|
|
Rodrigo Pesantez, MD
Orthopaedic Trauma Fundacin
Santa Fe de Bogota - Colombia
Date: Mon, 26 Jun 2000 14:21:24 +0800
From: efont
Dear Rodrigo,
Consider fusion of the ankle joint. this is going to be a very painful ankle if you try to salvage it by any other means.
Date: Mon, 26 Jun 2000 10:24:30 -0400
From: Charles Mehlman
Clearly the "health" of your soft tissue envelope is still of paramount importance and will strongly influence the success or failure of whatever treatment option you choose for your patient.
The thoughts I would submit for consideration are primary arthrodesis (pan-talar type procedure) versus TALECTOMY. In the setting of arthrogryposis, long-term (avg 10 years) results have been good regarding plantigrade feet with good walking ability. Spontaneous fusion also tends to occur.
I would further recommend Dr Tscherne & Dr Schatzker's book regarding such injuires: MAJOR FRACTURES OF THE PILON THE TALUS AND THE CALCANEUS, Springer-Verlag 1993.
D'Souza H, et al. Talectomy in Arthrogryposis: Analysis of Results. J Peditr Orthop 18:760-764, 1998.
Zwipp H. Severe Foot Trauma in Combination With Talar Injuries. IN: Tscherne & Schatzker [eds] Major Fractures of the Pilon the Talus and the Calcaneus. Springer- Verlag 1993. pp 123-136.
Raaymakers ELFB. Complications of talar Fractures. IN: Tscherne & Schatzker [eds] Major Fractures of the Pilon the Talus and the Calcaneus. Springer- Verlag 1993. pp 137-142.
Charles T Mehlman, DO, MPH
Division of Pediatric Orthopaedic Surgery
Children's Hospital Medical Center Cincinnati
Cincinnati, Ohio
Date: Mon, 26 Jun 2000 17:38:38 -0400
From: J. Tracy Watson
This would be a very difficlut ankle to fuse....In these situations we have resected the talar body and saved the head and neck of the talus if possible....then performed a tibial-calcaneal fusion as well as fused the talar head and neck to the anterior distal tibal region....stabilize the fusion (s) with screws and an Ilizarov type foot frame.....to avoid excessive shortening a proximal tibial corticotomy is performed to restore axial length....we leave the limb approx 3/8 to 1/2 inch shorter to accommodate a rocker bottm shoe.......in cases where the comminuted talar body may be infected....we do this as a staged procedure....resect the talar body , debride distal tibia and implant Antibiotic spacer.....come back at later date for fusion, frame and lengthening.
JTW
Date: Tue, 27 Jun 2000 15:36:50 +0600
From: Alexander Chelnokov
Hello J.,
JTW> the talar head and neck to the anterior distal tibal region....stabilize the fusion (s) with screws and an Ilizarov type foot frame
IMHO screws are superfluous here if anyway Ilizarov type fixator is used. If at least a two pair of wires are inserted (into calcaneus and distal tibia) it is quite enough to provide stability even more than needed.
JTW> .....to avoid excessive shortening a proximal tibial corticotomy is performed to restore axial length....we leave the limb approx 3/8 to 1/2 inch shorter
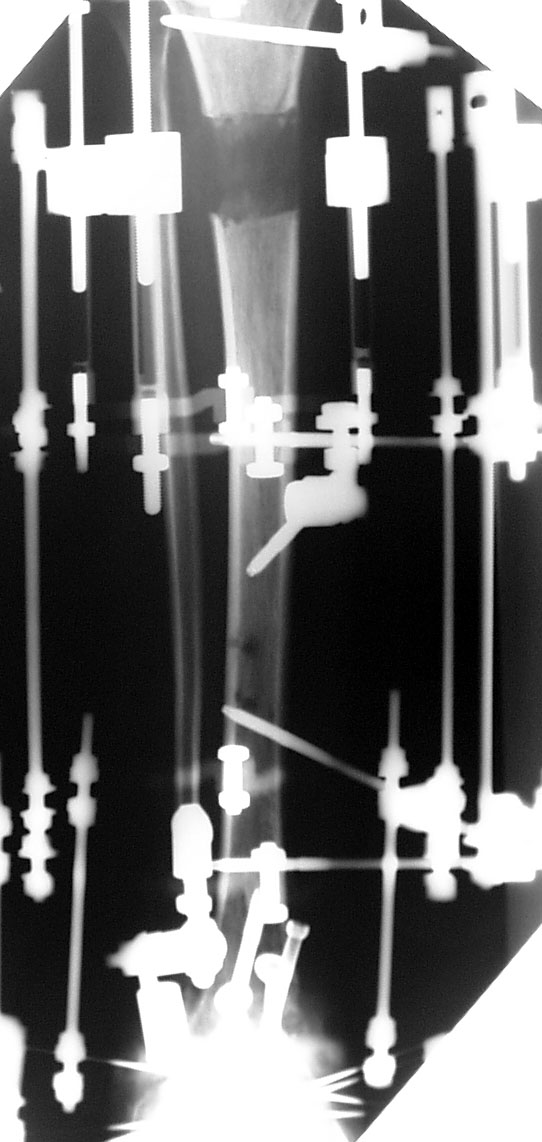
Lenghtening at two levels provides more short period of fixation. I already presented here such a case with 4 cm total lengthening. I attached the images as a collate. Failed to recover date of the last image.
 |
Best regards,
Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, Ekaterinburg, Russia
Date: Tue, 27 Jun 2000 06:41:56 -0400
From: J. Tracy Watson
TO A.C.
Agreed.....that the screws are superfluous......except that in our patient population they will not walk or tolerate a foot frame for any length of time...the screws allow us to remove the foot portion of the frame within 6 weeks....and that way they just have to deal with the tibial frame only....agree .. 2 corticotomies reduce total time in frame.
Date: Tue, 27 Jun 2000 07:15:54 -0400
From: E F Barrick
I would leave it in the external fixation for 2 to 3 months. This would give lots of time for the soft tissues to quiet down and heal. Then see how the patient does. You may be surprised that they can function. If not, then fuse it if there is enough bone stock. I have seen some nasty pilon fracture and talus fractures do Ok without further intervention.
Fred Barrick
Date: Tue, 27 Jun 2000 18:21:13 +0600
From: Alexander Chelnokov
Hello J.,
Tuesday, June 27, 2000, 4:41:56 PM, you wrote:
JTW> population they will not walk or tolerate a foot frame for any length of time...the screws allow us to remove the foot portion of the frame within 6 weeks...
It's fine! What screws are you talking about, how many and where they should be inserted? It is very good option though demands of our population maybe lower and they do tolerate the foot frame as much as needed.
When the tibiocalcaneal fusion was discussed here previously, it was stated that pantalar fusion is very worse option resulting with a lot of further problems. Are there any news about talar replacement?
Best regards,
Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, Ekaterinburg, Russia
Date: Tue, 27 Jun 2000 16:33:25 -0400
From: J. Tracy Watson
AC
See attached images which will hopefully answer your questions......
 |
 |
 |
 |
JTW
Date: Wed, 28 Jun 2000 17:42:05 +0600
From: Alexander Chelnokov
Hello J.,
THX, i got the idea. Do you then remove the screws? Though we don't have such cannulated screws in our OR, so this approach i'll keep in mind for future times of prosperity...
Best regards,
Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, Ekaterinburg, Russia