

Date: Sat, 17 Jul 1999 19:30:23 +0530
Subject: Neglected fracture dislocation hip
Dear All,
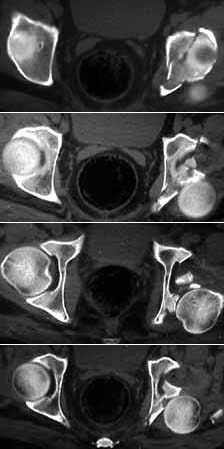
Seeking advice on management of 50 years old male who presented with infected fracture dislocation right hip with complete sciatic nerve palsy three months after injury. Xrays initial and current and CT scan Current images attached.
He was involved in a RTA about 3 months ago and underwent open reduction unsuccessfully followed by traction,elsewhere. The wound became infected. He came to me about a week ago in poor general condition with sinuses discharging pus. The sinus was explored. It led to the joint. The articular cartilage of both acetabulum and femoral head is completely destroyed. The posterior wall of the acetabulum was deficient and hip could not be reduced. Loose pieces from the joint were removed. Post op patient has been mobilised with frame. The sinus is slowly healing.
How do I salvage this hip ? Is there any chance of successful THR ? Any advice welcome.
TIA - Rajat Varma FRCS, Indore, India.
|
|
|
Date: Sat, 17 Jul 1999 08:00:51 -0400
From: Frederick Barrick, MD
Arthrodesis is still a good operation, suited to just such a situation. Girdlestone is the other viable choice. For a 50 year old I would opt for the fusion.
E. Frederick Barrick, MD
Date: Sun, 18 Jul 1999 09:25:57 +0500
From: Alexander Chelnokov
You could try to perform closed fusion of the hip using external fixator - as you reported joint surfaces have already been "prepared" by infection process. A pelvic frame with femoral extension can be used to reduce femoral head to the acetabulum gradually and then provide compression-stabilization. Obviously that any local implants are likely to be infected.
Best regards, Alexander N. Chelnokov, Ural Scientific Institute of Traumatology and Orthopaedics, Ekaterinburg, Russia
Date: Mon, 19 Jul 1999 13:26:38 -0600
From: Thomas A. DeCoster M.D.
Regarding patient with irreducible posterior hip dislocation, comminuted posterior lip acetabular fracture, postoperative infection with sinus tracks and complete sciatic palsy:
I am not certain why the hip is irreducible. The images show the femoral head completely posterior to the acetabulum with lots of bone fragments (presumably from posterior lip of acetabulum) anterior to the head nearly filling the acetabulum. You said bone fragments were removed. I would do whatever it took to reduce the head back into the socket.
The sciatic nerve injury may be the patient's biggest problem. It could be from initial injury, iatrogenic injury even laceration during first or subsequent procedures, or chronic traction from the posteriorly dislocated head. After obtaining hip reduction I would explore the sciatic nerve to make sure it is in continuing from the greater sciatic notch to the lesser trochanter.
An external fixator keeping the head reduced may very well result in a fusion. You might ream the acetabulum (total hip reamer) and ream the cartilage off the femoral head (THARIES reamer) if necessary and the bone isn't too soft.
Tom DeCoster, University of New Mexico, USA