


Date: Sun, 1 Jun 2003 13:47:28 +0000
From: Jeff Richmond
Subject: Ipsilateral Post Hip Fx-Dislocation + Femur Shaft Fx
I'd appreciate any input on this case- what to do now and would anybody have done anything differently:
65 year old obese male insulin dependent diabetic came in 3 nights ago- intoxicated driver vs tree. Face hit the windshield but head CT negative. Intubated on arrival. Ipsilateral midshaft femur fracture with a comminuted posterior wall acetabulum fracture/dislocation.
Base deficit was 10 and he was in diabetic ketoacidosis. About 5 hours later his base deficit was 15, although hemodynamically he was doing better. The general surgeons agreed to let me take him to the OR for a zero blood loss procedure. My thought was to ex-fix the femur to allow me to reduce the hip, and come back today and fix the acetabulum and antegrade nail the femur at the same time. After ex-fixing the femur, I was unable to get the hip reduced. The head came down, but would not seat in the acetabulum. I checked and rechecked the rotation of the femur fracture which looks fine. He went back to the ICU in skeletal traction, and is now 3 days out. Yesterday he was put on pressors and appeared septic. I have been unable to get him to the CT to see what might be blocked the hip reduction. This morning he is still on pressors, but far less than yesterday.
What now- Obviously I won't be able to touch him for at least a few more days. My concerns now are having soupy ex-fix pins in the Kocher-Langenbeck incision field. Someone suggested taking the frame off as soon as he is stable enough and retrograde nailing the femur and doing the acetabulum afer a few days to let the pin sites "cool off" but I am concerned about pounding a nail from below and damaging his femoral head and nerve more than they already are.
Any advice will be appreciated.
Jeff Richmond
North Shore University Hospital
Manhasset, New York
Date: Sun, 1 Jun 2003 10:19:25 -0500
From: J. Tracy Watson, M.D.
Would suggest a smaller diameter nail..so that you don't have to "pound it"..so hard......also perform with a femoral distractor in the intertroch area spanning into distal femur so that the distractor is protecting the head and nerve to some extent.....smaller diameter nail might not heal as well....so make sure that the nail is seated appropriately in the intercondylar area such that in the future... if you need to exchange nail...it won't be a flail...to get the rod out....just make sure it is seated elow the joint line ..but not placed way proximal in the intercondyalr region...such that it's a bear to remove....
JTW.
Date: Sun, 1 Jun 2003 17:53:49 -0600
From: Terry Finlayson
I would have elected a retrograde femoral nail initially through a patellar-splitting 3cm incision (minimal blood loss). At this point, I would do the same (retrograde IM nail) and overream by 2mm so you don't have to "pound" the nail into place. With the femur stabilized the acetabulum is easier to temporize with traction (proximal tibial pin) while the patient becomes more metabolically stable and the pin sites heal.
Terry I. Finlayson, M.D.
Alpine Orthopaedic Specialists
2380 N. 400 E. Suite A
North Logan, UT 84341
Date: Mon, 2 Jun 2003 08:32:24 -0400
From: James Carr
I'll bet his hip is reducing, but he has a huge posterior marginal impaction, and it slips right back out. I would not worry about the nail insertion screwing up his femoral head, especially if done retrograde. Put in a nice big reamed one. Pound away. And if you are worried about soupy pin sites for the hip approach, I would have the same reservations for the nailing. The literature on staged ex-fix- nail suggests you can wait for up to 2 weeks and avoid an increased infection rate. Ideally, both could be handled through the Kocker-Langenbeck. You can do him lateral decubitus, and won't need a fracture table to antegrade nail the femur. I have a poor track record with diabetics and ORIF of this type of acetabulum fx. They tend to be osteoporotic, and comminuted. If he has a large marginal impaction (ie most of the posterior wall), I would think about a retrograde nail, and come back on a delayed basis when he is better, and do a primary hip replacement. So for me, choice # 1 is do both through the hip incision. Choice #2 is retrograde nail the femur, and do whatever is appropriate for the hip on a delayed basis.
James B. Carr, MD
Palmetto Health Orthopedics
Date: Mon, 2 Jun 2003 07:22:47 -0700
From: Chip Routt
Please send along some films and a pelvic CT so we can give you opinions based on his specific information, rather than our guessing.
You want input, we want info-
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
325 Ninth Avenue
Box 359798
Seattle, WA 98104-2499
Date: Tue, 3 Jun 2003 01:51:21 +0000
From: Jeff Richmond
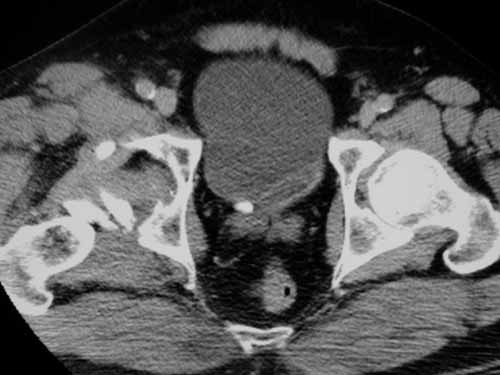
Here are the films. Sorry they weren't shown sooner.
|
|
|
|
 |
This discussion may prove to be academic - he is spiking to 40c on broad spectrum abx.
Thanks
Date: Tue, 3 Jun 2003 08:44:03 -0700
From: Chip Routt Thanks for the selective information.
There are many effective ways to treat this patient and his injuries.
His hip reduction is obstructed by fracture fragments and requires open
treatment, usually acutely. His femoral shaft fracture appears uncomplicated
with associated neck fracture or other nuisance, and one film shows a
proximal external fixator pin...so he must be in a lateral femoral frame
now.
As soon as possible, remove his frame, reduce and stabilize the hip, and
nail the femur. I'd do all procedures with the patient positioned prone on a
radiolucent OR table using a single prep and drape for efficiency. I'd
choose a K-L exposure for the hip, then antegrade, "not-too-much" reamed,
static locked nailing. You can use the lateral patient position if his spine
is cleared, and if you like. Prone protects a "non-cleared" spine, and
facilitates pulmonary improvement and operative imaging.
When you remove the frame initially, please leave the pins "in-femur" while
you fix the acetabular fracture. For several reasons - the destabilized
femur will relax the nerve, the pins can serve as proximal and distal
femoral fragment "manipulators", and just in case he has intraoperative
"issues" which delay the nailing to another time. When you begin the
nailing, back the pins out to the unicortical level so the medullary guide
pin, reamers , and nail can pass while the pins manipulate and hold the
shaft reduction.
Debride the necrotic caudal gluteus minimus muscle, wash the wound, and
close. Excise, thoroughly debride, and close the pin sites if you get to him
sooner than later. You might strongly consider some form of HO prophylaxis.
The sustained dislocation doesn't necessarily doom the femoral head, but
that coupled with his diabetes are significant risk factors.
Be safe, but be speedy. Keep it detailed, yet as simple as the situations
allow.
Sooner/faster is better than later/slower-
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
325 Ninth Avenue
Box 359798
Seattle, WA 98104-2499