


Date: Mon, 10 Jan 2005 19:32:19 -0500
From: Jeff Richmond
Subject: Acetabular Fx - both columns
|
|
|
 |
 |
Thanks in advance for any guidance on this case.
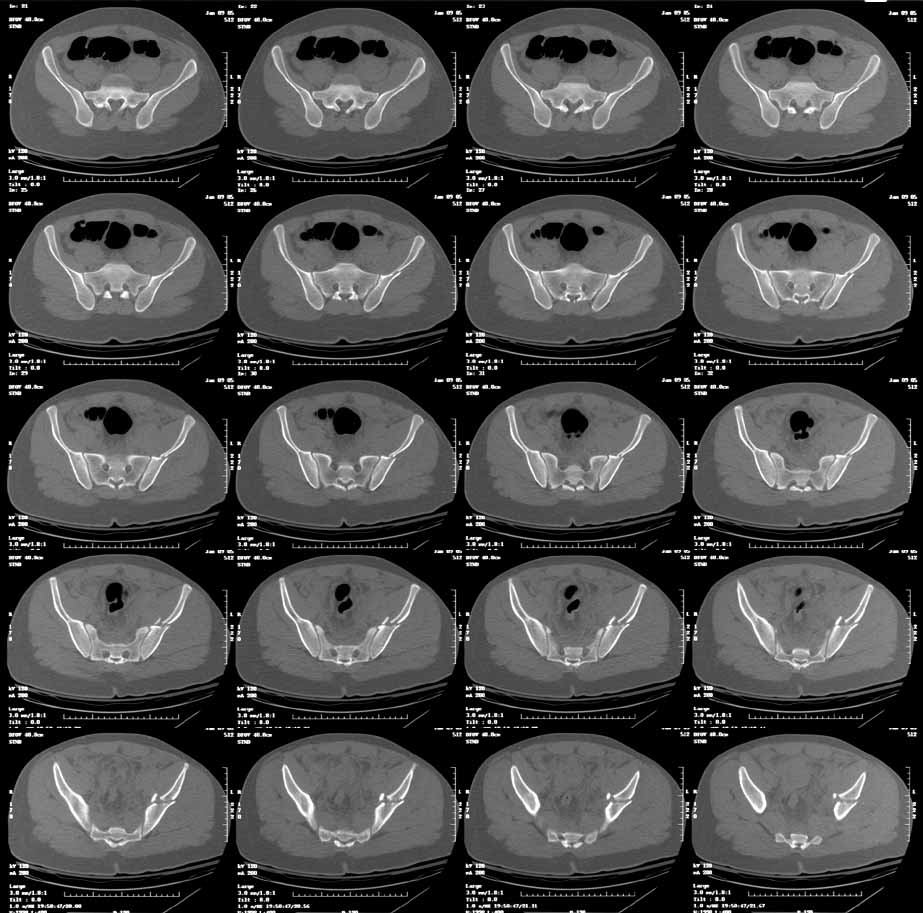
This is an 18 yo male involved in an MVA 2 days ago. Isolated injury other than some rib fxs. I had trouble interpreting the xrays, but the CT shows a both column fracture with secondary congruence (I think). The plain films show significant gapping of the anterior column, but the CT shows fairly little at the dome.
Reducing the anterior column should be straightforward through the ilioinguinal approach, but will the piece of the posterior column articular surface go with it, and if it doesn't will this be reducible after reducing the anterior component? Or is this true secondary congruence and what are the consequences of letting it heal as is?
Thanks
Jeff Richmond
Date: Mon, 10 Jan 2005 21:29:12 -0500
From: Bruce Ziran
Sometimes you can expose the outer ilium along the lateral window, a sort of extended II approach and sneak a recon plate that is over contoured as a spring/push plate and if the fragment is superior enough, maybe a percutaneous screw. Otherwise if critical to stability and reduction, got to bite the bullet and go from back also.
BZ
Date: Tue, 11 Jan 2005 07:49:57 -0800
From: Chip Routt
Thanks...your questions are good.
Yes, the posterior column dominant fracture fragment will follow the anterior column. Some surgeons would concentrate on the articular reduction and tolerate the slight residual medial displacement of the hip from the intact ilium. Both can be improved.
You'll notice by CT that there is an intact labral "hinge" which usually indicates that these 2 dominant articular fragments will behave together intraop. But you'll still need to expose, clean, and clamp them before fixation. And your operative goal is to have the articular reduction be perfect on the postop CT...can you make this one better?
There is no need for an ilioinguinal exposure for fixation in-situ .
The consequences of letting it heal as is are unknown but I'll tell you this...many postop CT scans don't look as good thru the dome as his does PREOP! You should really understand what you have and what you will do to improve it...maybe that's why you sent it, eh?
You'll notice that the anterior column is incomplete peripherally...this lends stability if you elect to treat him without surgery, and indicates an osteotomy at the iliac crest to complete the fracture and allow its mobilization for cleaning and reduction, should you choose surgery.
In 2005, there is no reason to struggle thru this alone. There are experienced acetabular surgeons very near to you who would do it or help should you choose to operate on him.
I think that a very experienced acetabular surgeon might operate on this fracture, and a less experienced surgeon would not...the result will depend on numerous variables.
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499
Date: Tue, 11 Jan 2005 14:05:08 -0500
From: James Carr
In my opinion, he will do well treated nonoperatively, and I have many similar cases in my practice with favorable followup. As Chip points out, the anterior column is incomplete peripherally, thus very stable in its current position. These are very hard to move intra operatively until the fracture is completed. Nonoperative Rx does carry a slight chance of further displacement, so close followup is needed. If I did anything operative, it would be a perc screw from anterior to posterior to secure the dome reduction. This can be done using the iliac wing view that profiles the "teardrop" to target the screw.
Jim Carr
James B. Carr, MD
Premier Orthopedic Specialists
Columbia, SC 29203
Date: Sat, 15 Jan 2005 16:22:31 EST
From: Stjmgja
We discuss in detail our operative approach.What are the specifics of your non-op treatment of this acetabular Fx? Skeletal traction- How much? how long? Bedrest how long? Non weight bear How long? Follow up XR how often ?
Thanks.
J Staeheli
Date: Sun, 16 Jan 2005 10:19:52 -0800
From: Chip Routt
Closed management is chosen when the fracture pattern and/or patient's condition allow.
For minimally displaced and stable fracture patterns in compliant patients without other mobility limiting injuries, we use no traction, unrestricted hip CPM as an in-patient, isometric exercises, and protected "weight-of-limb" bearing for 6-8 weeks. Weekly radiographs are recommend for the first 2 weeks after injury. You can always reassess your decisions during this phase if changes occur.
If non-compliance is anticipated, distal femoral skeletal traction can be considered.
For displaced or unstable fracture patterns in a patient not fit for surgery, we use distal femoral threaded pin skeletal traction for 6 - 8 weeks. Portable radiographs in traction can be obtained by a mobile unit if you choose. Adjustments can be made based on those films accordingly.
An exam under anesthesia and fluoroscopy can be used to help evaluate fracture stability if necessary.
The weight of traction selected is based on the films and/or exam under anesthesia/fluoroscopy...typically 10-15# for most patients.
Displaced and/or unstable fractures are operatively reduced and stabilized if the patient's condition allows.
I haven't used bedrest.
I haven't used "non-weight" bearing due to the greater forces on the hip when suspending the limb actively.
If in traction, the patient can have portable xrays using a mobile unit to avoid numerous transports for clinic visits. The clinic visit can then be at the 6 weeks anniversary, or sooner if the distal femoral threaded pin has "issues".
Pin care is simple with saline or peroxide 2-3 times daily, a dry dressing, and while keeping the skin edges free from serous crusting.
There are always numerous variables to consider when making such management decisions, but that's about it-
Chip
Date: Mon, 17 Jan 2005 08:16:00 -0500
From: James Carr
Since the injury has been judged to be stable, the patient can get out of bed, foot flat gait. I would repeat plain films in 3-4 days, and repeat the Cat scan at 7-10 days. If the patient is not comfortable with this plan, he gets fixed. Most are glad to avoid an operation.
Jim Carr
James B. Carr, MD
Premier Orthopedic Specialists
Columbia, SC 29203
Date: Mon, 17 Jan 2005 12:05:49 -0800
From: Chip Routt
Why do you repeat a CT scan?
Do you obtain it in or out of traction?
If "in", how do you rig that to maintain traction while travelling thru the machine?
If "out", what information do you get from the scan?
Who pays for the 2nd CT scan?
Chip
Date: Tue, 18 Jan 2005 08:48:25 -0500
From: James Carr
Chip
The repeat CT is admitted over testing in many cases, and will be omitted on a case by case basis. It makes me feel better about the choice (treating the doctor??), and also reassures the patient. Insurance or the hospital picks up the tab. In the case presented, the price of a CT is a small amount for a hip with 60 years ahead of it. My recommendation is likely the result of a medical legal scars from my days in Chicago where I had 5 lawsuits as a resident. We were taught "don't try to save the patient money, because it will wind up costing (you) a whole lot more than any test ever could". I do not repeat them in traction cases (rare nowadays) because of the logistics that you mention. We have largely abandoned femoral pins for small, smooth wires in the proximal tibia.
Jim Carr
James B. Carr, MD
Premier Orthopedic Specialists
Columbia, SC 29203