Date: Sat, 29 Sep 2001 11:17:23 -0700
From: John Ruth
Subject: Maluniting pelvic ring injury
2 days ago I was asked by a local rehab hospital to evaluate a 21 yo female
who while visiting out of town was thrown from a walk bridge (fall 20-30 ft).
She sustained a left sided lateral compression pelvic ring injury and a fracture
dislocation of the left elbow. The injury occurred on 9/1/01 and the treatment
of her pelvic injury was skeletal traction and the elbow was splinted only (now
subluxed with a comminuted radial head fracture and no motion). Her elbow is a
priority a will be addressed.
She is very petite (95 lbs. And 5 2) had no
other significant injuries specifically no lower extremity nerve injuries. She
has been at bed rest in traction since injury. Clinically she has 2 cm leg
length discrepancy (LHer radiographs demonstrate what I think is inward and
upward rotation of the left hemipelvis with radiographic confirmation of the leg
length discrepancy. There is obvious callus at the rami fracture sites and there
is no clinical motion of her pelvis. I have removed her traction and mobilized
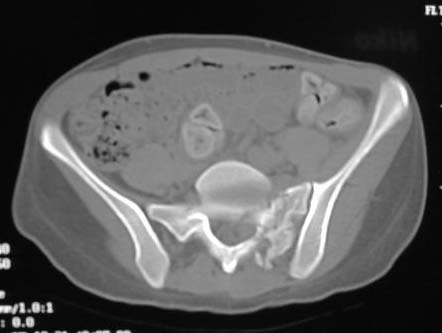
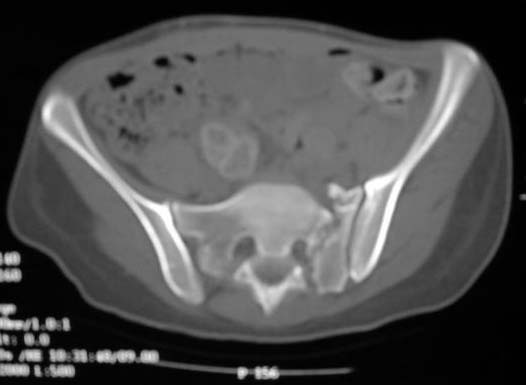
her out of bed. I am considering addressing the maluniting pelvic injury. Her
CT shows an impacted zone 1 sacral fracture with callus. Images will be sent in
additional mailings due to size.
Questions:
1. Is it reasonable to consider take down of the uniting fractures with
probable osteotomy of the left sacrum and internal fixation to restore the leg
lengths and likely future sitting balance?
2. Considering J Mattas recommendation (CORR 1996) of 2 or 3 stages, is
it reasonable to try and perform this in one stage using a bilateral ilioinguinal
aproach to mobilize the rami fractures, do an anterior osteotomy of the left
lateral sacrum preferably through the fracture site, reduce the left hemipelvis
using an appropriately placed femoral distractor and internally fix the rami with
a solitary spanning anterior plate and the sacrum using a percutaneous fully
threaded cannulated screw? Obvious concerns include damage to the L4, L5 and S1
nerve roots. SSEP is planned but certainly not fool proof.
3. Any other thoughts or recommendations?
 |
 |
 |
| AP |
Inlet View |
Outlet View |
Reply at: Orthopaedic
Trauma Association forum
Date: Sat, 29 Sep 2001 14:09:04 -0500
From: Marc F. Swiontowksi, M.D.
John - in my opinion you cannot "mobilize" the scral injury from the anterior
approach without a very high risk of L5 and possibly S1 injury. Recommend
mobilizing the sacrum via posterior approach, leaving it unstabilized, then
supine with ilioinguinal approach with distal femoral tration pin.
Stabilize with iliosacral screw in supine position after plating anterior
ring injury- you may be able to avoid leaving the contralateral anterior
ring injury without internal fixation depending on the overall correction
of length and malrotation of the ipsilateral posterior ring injury you
obtain. Huge case but at least she is tiny. Good luck
marc
Date: Sun, 30 Sep 2001 21:57:01 +0100
From: rajesh
If the limb length discrepancy is only 2 cm ,and she has no other
problems,can this not be sorted out by giving a shoe raise rather than a
pretty major surgical procedure with a very real risk of neurovascular
damage?
Mr.K.Rajesh,MS(orth),DipNB(Orth),FRCS,FRCS(Orth)
Hope Hospital
Salford, UK
Date: Sun, 30 Sep 2001 08:12:01 -0500
From: Adam Starr
Howdy.
I think it IS reasonable. As long as she knows that there's a risk of
neurologic injury, and she agrees to go ahead, I think it's the right thing to
do.
I'd try to do her pretty soon. It will be easier to find and mobilize the
healing sacral fx from the back the sooner you do it.
I would approach the sacral fx posteriorly and mobilize it first. It's going
to be tough to know when enough is enough in the back. The healing rami won't
give you too much motion, even if the back is loose. Hopefully you'll be able to
tell that you're close in the back by rolling the sacrum down and checking the
image. Nice thing about the open approach is that you'll be able to look directly
at the fracture surfaces, too.
Then I'd close the posterior wound and put her supine to address the anterior
ring. The left ramus fracture looks like it might be mobile now, but the right
one has quite a bit of callus - I doubt you'll be able to move it.
Up front, I'd do what I had to to get the rami mobilized. You could do this
through an ilioinguinal bilaterally. You might be able to get the same amount of
motion by using a Stoppa. I think freeing up the anterior ring will probably be a
little easier than the posterior ring, but maybe you'll find otherwise.
We don't use nerve monitoring down here.
For fixation, I agree with the choice of iliosacral screws. I would choose
screws up front, too. I like them better than plates.
These are always tough cases. Good luck to you.
Adam Starr
Dallas
Date: Tue, 2 Oct 2001 18:41:23 +0600
From: Alexander Chelnokov
Hello John,
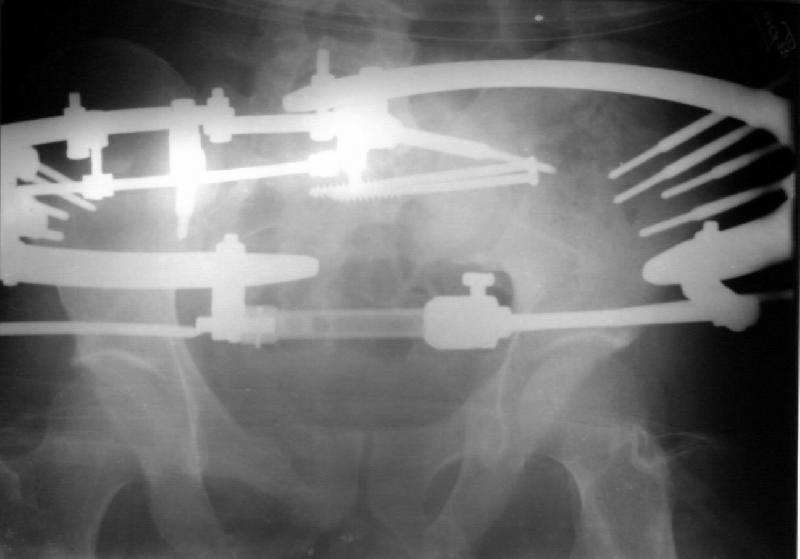
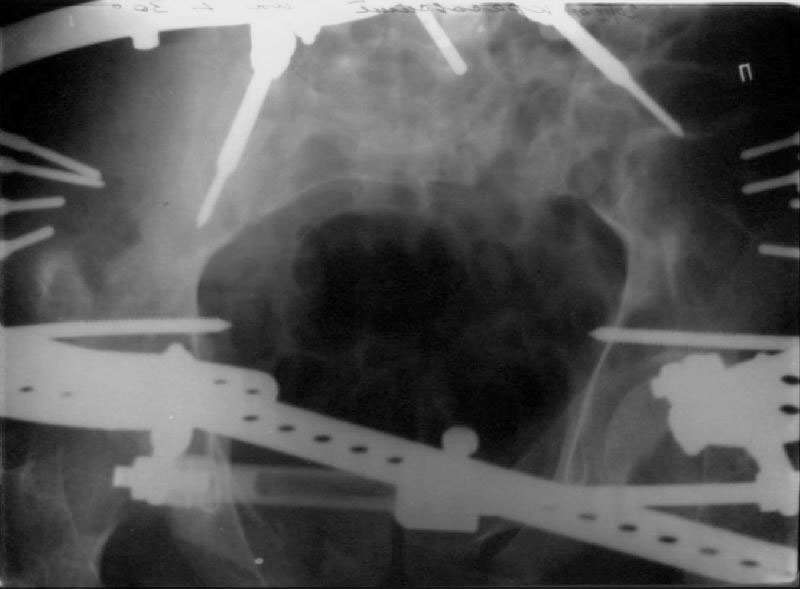
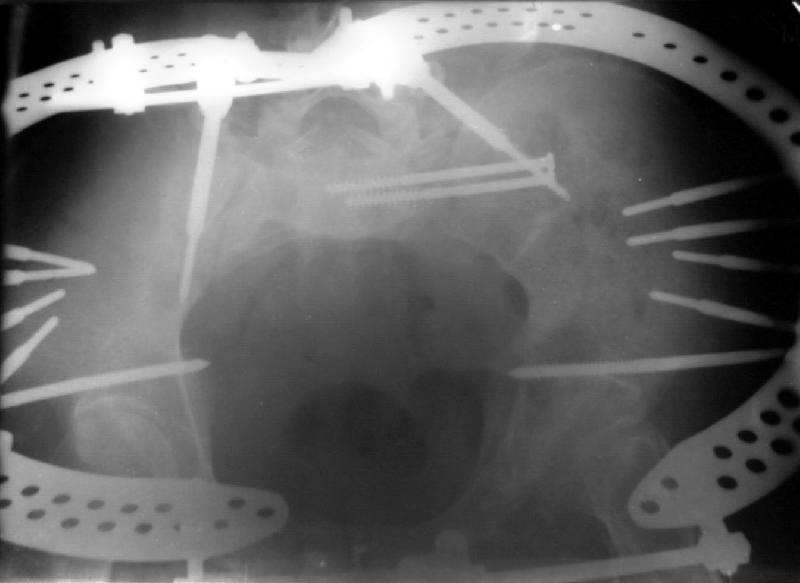
An example of our current approach to similar injuries - A 26 y.o.
male admitted to us Aug 23, 2001 6 weeks after injury (compression by
a wheel of a truck).
An external fixator was applied and gradual reduction was started -
lateral traction to mobilize sacral fracture and then the hemipelvis
was moved downward. Then lateral compression was performed.
Yesterday iliosacral screws was inserted.
The last couple of images are skewed, they were made in OR and patient was not
properly positioned.
 |
 |
 |
| AP - 6 wks s/p Injury |
AP - lateral + distal txn |
AP - iliosacral screws |
 |
 |
 |
 |
| Inlet - 6 wks s/p Injury |
Inlet - lateral + distal txn |
Inlet - lateral compression |
Inlet - iliosacral screws |
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Tue, 2 Oct 2001 10:23:25 -0700
From: John Ruth
Thanks for the images. Did you do any form of open osteotomy prior to the
initiation of distraction?
Date: Wed, 3 Oct 2001 00:14:42 +0600
From: Alexander Chelnokov
Hello John,
No, this case is managing closed.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Mon, 8 Oct 2001 16:32:11 -0700
From: John Ruth
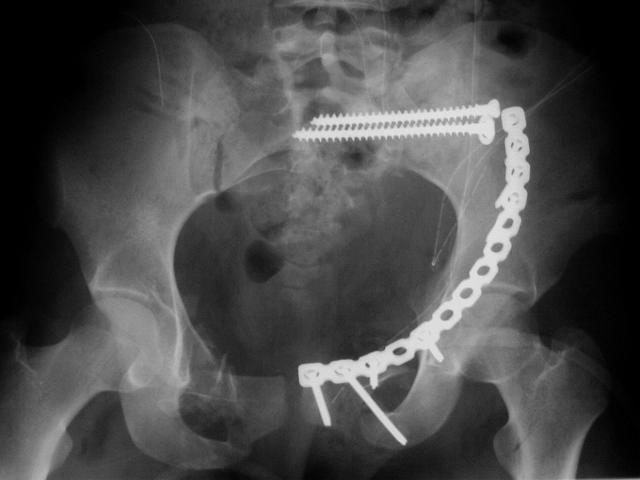
I did as suggested, I performed a 2-stage procedure (posterior sacral
osteotomy and anterior take-down of left-sided rami fractures and anterior plate
and percutaneous iliosacral screw fixation). It was a difficult and humbling
experience. I felt as though the sacral osteotomy was complete and seemed so
using intraoperative image views (inlet, outlet and true lateral of the sacrum)
however after placing the distractor anteriorly I found that I could not see the
sacrum well due to the bulk of the distractor itself. I then replaced it with
radiolucent external fixation bars and noted widening of the left anterior SI
joint.
Apparently my sacral osteotomy was not complete and the rotational
correction (lateral and inferior) was occurring through the SI joint, at least
anteriorly. An intraoperative x-ray showed definite improvement of the leg
length discrepancy but not complete. I felt that in addition to the rotational
correction the left hemipelvis also needed to move inferior as well. Due to the
patient's small size, traction on her left leg simply produced pelvic obliquity
and I really did not have a way of placing well leg traction which would require
a post and at the same time obtain adequate intraoperative image views. Long and
the short is I accepted a less than perfect reduction but with leg lengths now
with less than 1 cm difference clinically and radiographically and I fused her
left SI joint. No post-op nerve deficits. It was definitely a learning
experience.
Any and all feed back is appreciated. Postop pics enclosed.
 |
 |
 |
| AP |
Inlet View |
Outlet View |
Date: Mon, 08 Oct 2001 19:13:15 -0700
From: Chip Routt
Hi John-
Thanks for being kind enough to share your patient's example both pre- and
postop. We all share your pain.
Probably the best treatment is avoiding this situation. Educate the
individuals involved in her initial evaluation. Teach them the importance of
clinical and radiographic patient evaluations. Teach them exactly how to examine
an injured pelvis. If it had been examined initially, the clinical instability
would have been obvious. The radiographs reveal bilateral, comminuted, displaced
anterior ramus fractures along with a sacral fracture which violates the
anterior, middle, and posterior portions of the sacrum (analogous to a complete
sacroiliac dissociation)....a "3 column injury"(if you pretend that the sacrum is
a vertebra), so to speak.
Early intervention allows: (1) manipulative corrections (using either open,
closed, or combination techniques) with accurate reductions and stable fixations
of your choice, (2) patient comfort, (3) improved pulmonary function, (4)
diminished neurological risk, and (5)early patient mobility.
Explain to them exactly why this matters.
These are difficult (mood breaking) late reconstructive operations as you
know. Thankfully, these are not so common, or we'd all quit.
You may consider this- (a) destabilize the healing anterior ring lesion(s),
for this patient both ramus fractures could be accessed using Stoppa exposures,
then close the wound, (b) insert a distal femoral traction pin then turn prone,
apply appropriate traction (can be simply hung over the edge of a radiolucent
table...nothing fancy), and then destabilize the sacral fracture (and contracted
soft tissue envelope) while preserving any and every dorsal sacral cortical
interdigitations, (c) slowly reduce the sacral fracture using an appropriate
manipulative clamp/device to correct length, rotation, flexion, translation,
etc...this may require a contralateral dorsal exposure of the posterior iliac
spine for secure "anchoring" of the manipulative device, or other
techniques...after reduction, carefully compress and secure with
fixation...iliosacral screws may be insufficient for this task dependant on
chronicity and deformity severity...maybe build to the contralateral posterior
iliac spine (consider this when anchoring the "manipulator" there since you may
need certain sites for fixation), or use Schildhauer's technique of "triangular
osteosynthesis" building onto the lower lumbar pedicles as well, and then (d)
turn supine and assess the anterior instabilities under fluoroscopy, then if
necessary (using the previous Stoppa exposures or other fixation techniques)
stabilize the unstable anterior elements.
Intraoperative fluoro can be misleading regarding deformity
corrections...maybe consider plain films when needed. Notice this lady's external
rotation of the left hemipelvis postop and its impact on the acetabular
coverage...see the inlet(caudal) view with attention to the ischial spine
assymetry.
Maybe consider referral to another regional surgeon, assuming he/she has
additional experience with such patient problems. Then travel with the patient
and scrub on the operation...maybe even to Russia to see Alex!!!!!...., but
she'll need 2-3 seats when flying home, one for her butt........... and 2 others
for her frames!
Sorry to not correspond earlier.
Chip
Date: Tue, 9 Oct 2001 08:47:03 -0700
From: John Ruth
Thanks for the advice. Unfortunately there isnt anyone else in southern
Arizona and I am not familiar with anyone with a lot of experience in Phoenix.
This patient is on the Arizona Medicaid system and really cant go anywhere
else. I plan to write the individual who initially cared for this patient.
Date: Tue, 09 Oct 2001 02:56:16 -0500
From: Adam Starr
John,
Excellent work on preserving the nerve roots. Every paper on outcome after pelvic
fracture points to neurologic function as one of the predictors of outcome - and
you preserved that, which isn't always easy.
Most of the papers on pelvic malunion I've read contain post-op pictures that
show imperfect reductions. It's good to strive for perfection, but it looks like
these cases are capable of humbling all of us.
I'd be curious to see how this lady does. If you get a chance, post some
follow-up info for us. Thanks for posting the case.
Adam Starr
Dallas, Texas