


Date: Fri, 18 Sep 2009 19:52:28 +0530
Subject: Multiple fracture left upper limb
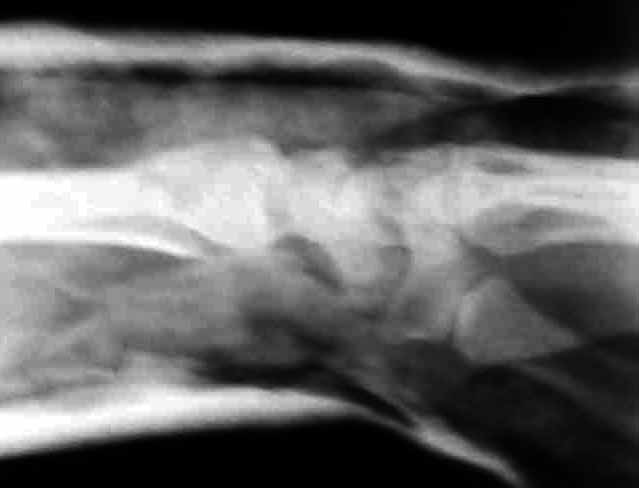
This 30 year old man sustained comminuted fracture shaft and undisplaced fracture neck of humerus. He has also technically compound fracture Distal Radius with intra-articular extension, but joint surface is congruent in the same upper limb. At present wound debridement POP immobilisation done. Options for management in this case? I am inclined to continue conservative management.
|
|
|
Dr Sathis Chandran
Koyili hospital,
Kannur, Kerlaa, India
Date: Thu, 18 Sep 2003 17:51:09 -0500
From: Obremskey, William T
Humerus can be treated w/o op in a brace. I would consider ex fix of wrist.
Bill Obremskey
Date: Thu, 18 Sep 2003 21:47:10 EDT
From: Aobonedoc
Hello:
I mostly likely would I & D the open distal radius followed by the application of an external fixator. Proximal humerus: most likely would treat nonoperatively. midshaft humerus fracture: possible nonoperative treatment although I might consider retrograde flexible nails such as rush rods (kind of old fashion but with luck might be able to able to insert all the way up into the humeral head).
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005
Date: Fri, 19 Sep 2003 19:51:45 -0600
From: Terry Finlayson
Given the multiple injuries this patient has sustained and the compound fracture of the distal radius, I would ex fix the wrist after appropriate debridement and surgically stabilize both humerus fractures to facilitate mobilizing this patient. I'm not usually a fan of violating the rotator cuff, but in this case an antegrade humeral nail with design allowing fixation of the proximal humerus (e.g., Polarus nail or similar) would stabilize the humerus adequately to allow early passive and active ROM of shoulder and elbow and, in my experience, would significantly decrease pain. Plate osteosynthesis is reasonable, but more OR time, bleeding and post-op pain; although it spares the rotator cuff.
Terry Finlayson, MD
Alpine Orthopaedic Specialists
North Logan, UT
Date: Sun, 21 Sep 2003 10:24:56 +0600
From: Alexander Chelnokov
Hello Satish,
s> debridement POP immobilisation done. Options for management in this case? I am inclined to continue conservative management.
It could be useful at least to apply an external distractor to the distal radius to maintain reduction. The humerus may be left in brace. Maybe it makes sense to place some perQ pins/wires to prevent displacement of the proximal fracture. In our settings closed nailing would be performed.
Best regards,
Alexander N. Chelnokov
Ural Scientific Institute of Traumatology and Orthopaedics
str.Bankovsky, 7. Ekaterinburg 620014 Russia
Date: Sun, 20 Sep 2009 18:03:19 +0530
From: satish
Dear all,
Presently I did closed reduction and Plaster cast immobilisation. Post reduction Xrays are attached. Do you think this will slip subsequently ?
 |
 |
Dr Sathis Chandran
Koyili hospital,
Kannur, Kerlaa, India