
Date: Fri, 5 Aug 2005 21:28:54 -0400
From: thomas schaller
Subject: nonunion of femur
Hello
May I have some advice on the following case?
Middle aged woman, No chronic medical problems, +tobacco use - but she promises she's going to quit!
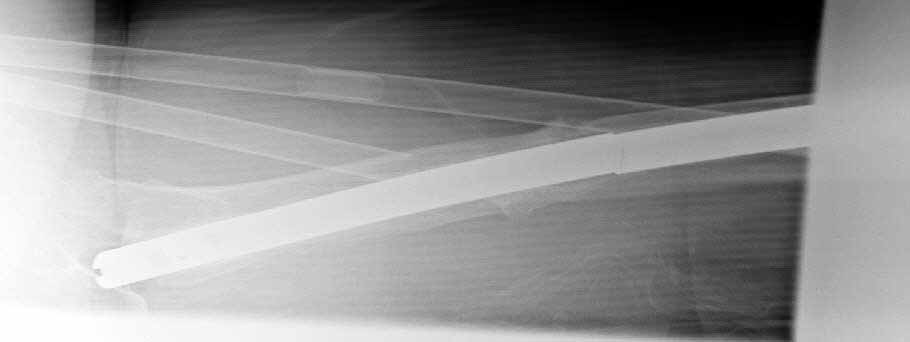
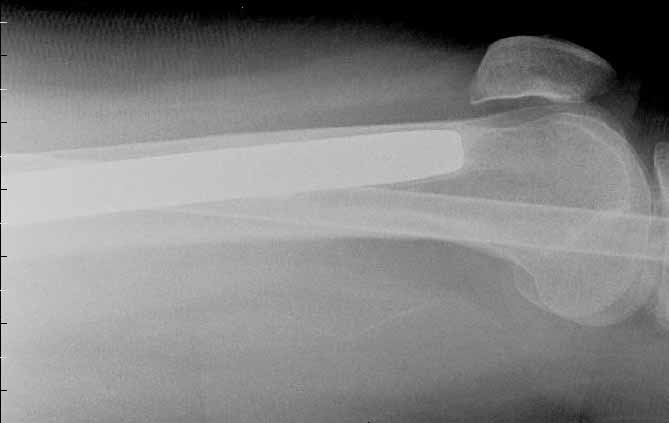
Original MVC in late 1990's, initial rod failed, and 2 subsequent exchanges failed (most recently shown in attached jpgs.) most recent one (6/2002) was apparently an open nailing to remove last broken nail, but no grafting was performed in conjunction.
|
|
|
|
Now sent to me with broken 14mm R/T nail in place.
WBC, Hgb, Chemistries normal
ESR 34
CRP 4.2
No other apparent locus of infection.
I was considering a staged approach - removing nail and screws and obtaining cultures.
If negative, proceed with exchange nailing with open grafting +/- BMP, But how best to deal with that pedestal distally and avoid anterior breech near patella?
If positive cultures, what would be best option?
Thanks
Tom Schaller
Kalamazoo, MI.
Date: Saturday, August 06, 2005 3:35 PM
From: Timothy Bray, MD
After three failed nailings, 4th doesn't sound great to me. Check for diaphyseal necrosis with bone scan/MRI, maybe prior surgery has left avascular zone, nutritional status, stop smoking, full medical work up for systemic disease. Convert to locked bridge type plating with autogenous bone graft. Keep her off for 8-12 weeks. If infected, IM debridment, temporary external fixation, IV antibiotics then above surgery when aspirate negative 6-8 weeks; if malignant organism she may loose the leg. Tough case.
From: Jeff Brooks
Date: Sun, 7 Aug 2005 17:22:39 -0400
Would this be totally off-base to try (IF she stops smoking entirely, which may be high hopes):
STG I: Remove nail, wide debridement, bone Cx, ABx beads as spacer, Tx presumptively for osteo (since her ESR & CRP are high there must be something brewing in there)
wait 6 weeks, tailor ABx to Cx results
STG II: vascularized fibula - into descending branch of the lateral circumflex femoral artery, with autogenous ICBG, +/- BMP7 and a long lateral locked plate??
Otherwise, I agree chances of amp seem high.
Jeff Brooks
Stamford, CT
From: Bill Burman
Date: Sun, 7 Aug 2005 11:58 PM
See Brinker MR, O'Connor DP. J Orthop Trauma. 2003 Nov-Dec;17(10):668-76. Ilizarov compression over a nail for aseptic femoral nonunions that have failed exchange nailing: a report of five cases.
If segmental resection is required for infection or avascularity, intramedullary bone grafting might be an option. See Winquist OTA BFC Lecture or Chapman JBJS 62A 1005 1980
Date: Mon, 8 Aug 2005 23:53:38 +0600
From: Alexander Chelnokov
Hello Thomas,
ts> Original MVC in late 1990's, initial rod failed, and 2 subsequent exchanges failed (most recently shown in attached jpgs.)
THX for sharing the extremely difficult case. Never met nail breakage at the level. Looks like the nail was never dynamized - is that so?
If no clinical signs of infection would be found during nail removal, i would still proceed with a solid titanium nail without site opening. Largest one we have available is 13 mm and it looks enough for most cases. Presumably you guys must be much more happy with implant choice than we here.
I would 1) use a poller wire to push the distal tip more posterior than it is now, 2) use a nail with extended options of distal locking (3-4 screws) and/or use poller screws - probably for the proximal fragment too, 3)lock it statically for 8-10 weeks, then dynamize by removal of the proximal locking screw. Good initial stabilization and no dead space in the nail must be enough to control low grade infection if any.
In case of pus in the medullary canal solution could be to perform debridement, take 10-12 mm rod, paste it over with AB cement, push through the 14 mm hole to have diameter equality, and insert it as temporary or maybe even definitive implant.
Good luck. Keep us informed.
Best regards,
Alexander N. Chelnokov
Ural Scientific Research Institute of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Thu, 11 Aug 2005 09:28:23 -0700 (PDT)
From: Djoldas Kuldjanov
I agree that avascular necrosis and infection should be ruled out at the level of the femoral nonunion.
The treatment of this femoral nonunion seems straightforward. Straighten the bone. Prepare the canal. Place a stronger, bigger nail. Dynamize and the problem is resolved. However, this idea was previously tried three times and the patient still has a femoral nonunion.
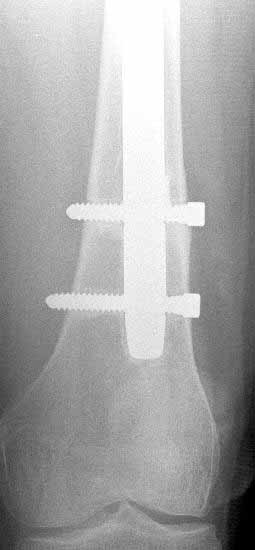
In my opinion, there is no nail strong enough to tolerate a varus deformity of femur after nailing. The AP view of the distal femur shows that the femur has been repeatedly nailed in varus. The tip of the nail is short and lateral in distal lateral metaphysis. It should be central over the intercondylar notch and buried in the distal epiphyseal scar. This has resulted in constant bending forces on the nail (see the "windshield wiper" sign) and its eventual fatigue failure.
|
|
|
|
I would first determine the degree of varus deformity with a long standing AP x-ray. After nail removal, irrigation, debridement and reaming of the nonunion, specimens would be sent for pathology and culture. If there was any sign of infection, placement of custom made antibiotic nail e.g.J Orthop Trauma. 2002 Nov-Dec;16(10):723-9. for two or three weeks would be performed before an ORIF plate fixation with Judet decortications and bone graft.
My first definitive treatment choice would be a long lateral tension band plate with insertion of proximal screws directed proximally at an angle of about 25-30 degrees. Correction of the varus would be accomplished by using a tensioning device distally or compressing with two eccentrically placed distal screws simultaneously as shown in Lawrence Webb's OTA BFC lecture or two distal screws directed distally. Fixation would be completed by a pair of locking screws each side of the nonunion.
My second choice would be an Ilizarov compression over nail if there is familiarity with both nailing and Ilizarov technique.
Djoldas Kuldjanov, MD
Department of Orthopedic Surgery
St. Louis University Medical Center