

From: Dr. Doe
Subject: APC III pelvis fx
Date: Sun, 27 Nov 2005 18:33:35 -0500
Hello gentlemen-
Case is 52 YO male, fell out of treestand while deerhunting.
He is 6 ft, approx. 260-275 lbs.
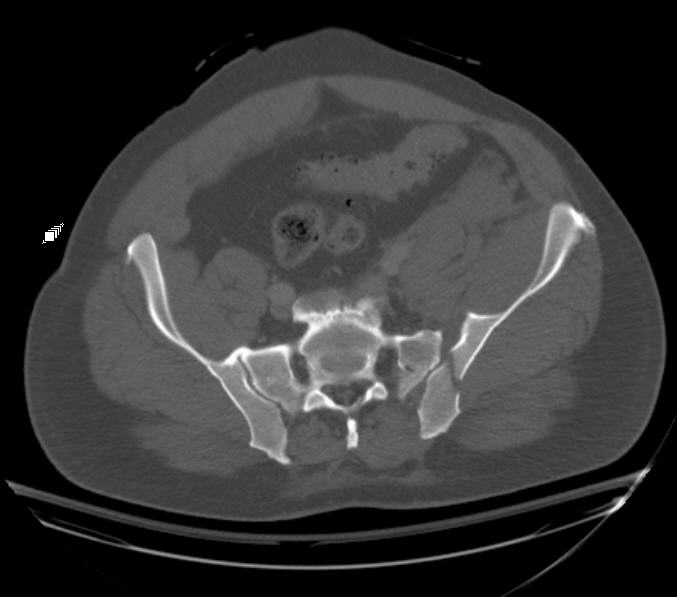
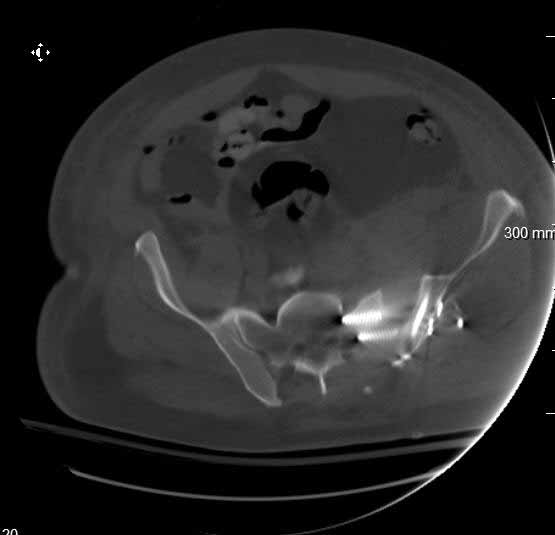
Was hemodynamic unstable at local ER, sent to our Trauma center where circumferential pelvic binder placed and pt. stabilized with fluid, blood, and rewarming. Angiography not performed. An extraperitoneal bladder disruption was found, uro elected to treat non-operatively. Initial xray (not shown) demonstrated 5-7 cm wide at symphysis and SI joint. The first image attached is of CT once binder is in place.
|
|
|
|
On post trauma day 5 the pt was taken to OR for ORIF of his iliac wing fracture and SI dislocation. The swelling/3rd spacing of fluid in the area of symphysis was profound, but quite acceptable posteriorly.
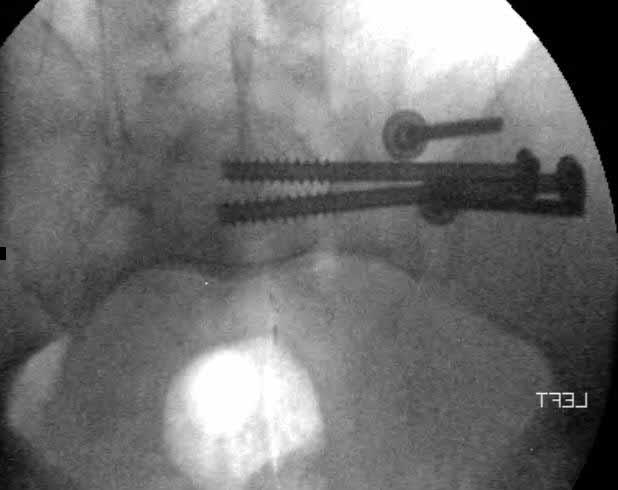
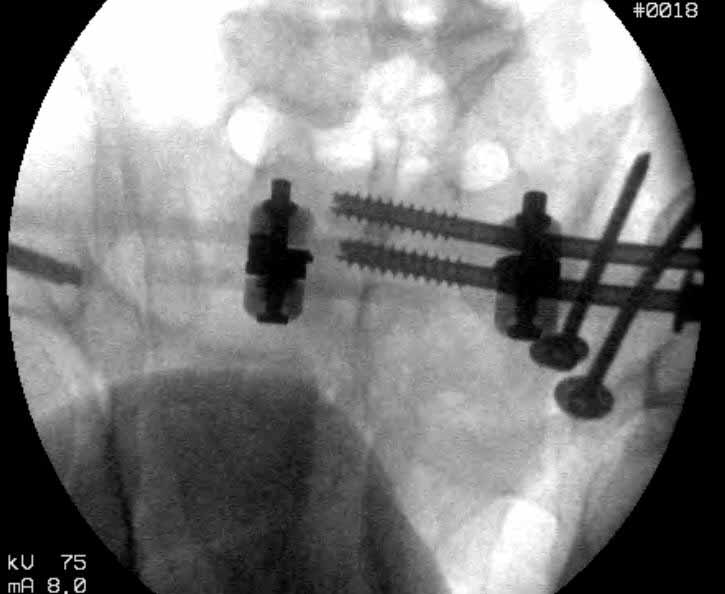
Patient was prone for procedure, as I thought too difficult to fix the wing in lateral position. Of course the repair of wing was easy, but reduction of SI very demanding. The Floro images document the residual lack of reduction. That was the closest I could get it using 6mm joystick in wing, and clamp on sacrum and clamp through notch. The fixation was (initially) rigid. Anterior ex fix with supra-acetabular pins was placed due to condition of soft tissues, massive "beer-belly" overhanging the crest.
 |
 |
 |
 |
 |
Post trauma day ten patient's xray shows failure of posterior construct. Plan was to perform revision orif once soft tissues resolve considerably for full anrterior fixation and posterior fixation. However, while Im away for holiday (on Post trauma day 15), pt is developing septic clinical appearance, and trauma suspects pelvic abcess near symphysis and performs I and D - finds nothing but no primary closure performed. Posterior tissues/incision continue to look healthy. Now is post trauma day 17, pt is still tubed/on dopamine/and wbc still elevated, anterior incision still packed open.
Clearly must get to bottom of possible sepsis, but then what?
Thanks for your time - sorry for such lengthy clinical description.
From: Adam J. Starr, M.D.
Date: Mon, 28 Nov 2005 11:35:32 -0600
That's a great case.
I'd stabilize the iliac wing fx first, then bring the ilium back into alignment with the sacrum. At our center, that would mean supine position, a perc LC 2 screw to stabilize the iliac wing, then a perc iliosacral screw to fix wing to sacrum.
The perc fixation's not so hard, but the reduction using closed or perc methods can be very tough.
Adam
From: barry berger
Date: Mon, 28 Nov 2005 20:46:26 -0500
For what it's worth, I recently had a similar fracture and found the reduction was far easier with an anterior SI approach despite significant patient size. I performed a primary fusion with iliosacral screws and although I was left with 2-3 mm of joint widening, he has done very well clinically and radiographically. I had initially plated the symphysis in this patient but found that the SI reduction was actually easier with no anterior pelvis fixation- any small amount of malrotation of a plated symphysis seems to make anatomic SI joint reduction difficult.
Good Luck.
Date: Mon, 28 Nov 2005 23:01:58 -0800
From: Chip Routt
It's hard to manage pelvic ring instability, and early decisions usually have dramatic impact on the result.
I don't think that this is "a great case"...it's a human, and it's a sad scenario.
Here are some observations, comments, and suggestions that are based on learning experiences-
1. Please consider strongly not waiting until day 5 to stabilize a patient with an unstable pelvic ring disruption...it makes no sense...if you can't get to it, transfer him urgently to someone who can and will.
2. Work with your urologists to coordinate bladder repair with early symphyseal reduction and fixation at the same anesthetic and exposure...if they don't want to play nicely, get your patient to someone with a urologist who will work on such injuries...this relationship is vital.
3. Reduction of the symphysis will improve posterior ring reductions for certain posterior ring injuries, especially if done within the first 2 days...you can always reduce and just clamp the symphysis, pack that wound, expose the SI joint anteriorly, reduce and stabilize it, return to the front and fix the symphysis, wash and close the wounds.
4. When you reduce such an iliac fracture-SI joint articular disruption using an anterior iliac exposure, you can use lag screws for the iliac component along with iliosacral screws (or a plating technique) for the SI joint component, similar to what you did from the back...the articular reduction is visible and predictable within the field...it's so much easier than clamping thru the notch and then feeling around hoping that it's reduced anteriorly while the body weight confounds your efforts.
5. Your caudal iliosacral screw is/was in his spinal canal...it's low and posterior and the lateral fluoro image confirms this...a postop CT will show it (or it's trail at this point)...canal screws do not hold.
6. Frames (even fancy new-style low ones) have poor mechanical stability when compared to symphyseal internal fixation...unstable rings in fat (and skinny) folks demand stable anterior and posterior stabilities...a frame can't get you there...consider it a helper/support at best.
7. A beer-belly does not complicate symphyseal reduction and fixation...it's just a deeper wound, and so you need a friend to hold a retractor or two....and if you can fluoro the patient's posterior pelvic ring intraop, he's not so fat!
8. If you are aware of the fixation failure before you vacate town, sometimes you just have to miss a holiday in order to help the patient...or at least have a plan to pass the patient along to a competent colleague to care for while you are away.
9. At this point, (if he's alive) get busy get a CT so you can understand what's happened, where the implants were, what fixation zones remain, remove the failed posterior implants, turn him supine, expose the symphysis and SI joint, reduce and clamp them both, fix them according to the CT info, close the wounds if clean, pack open if not, get another CT to assure adequate reductions and implant safety, treat his wound culture results with appropriate antibiotics, and nourish him.
I'm very sorry for you and the patient that this has happened, thank you for sharing it, and considering the above.
I hope that he can survive-
Chip
Date: Thu, 01 Dec 2005 15:39:00 -0800
From: Chip Routt
What did you do?
From: Dr. Doe
Date: Thu, 1 Dec 2005 22:07:04 -0500
On 11/29 took patient back to OR and explored both his anterior and posterior wounds, removed loose illiosacral screws. Left behind the screws fixing illiac crescent. Found anterior wound clean and closed it. Found posterior wound with moderate seroma and some adjacent fat necrosis. Thus far, cultures negative, but not kidding myself on that fact. Wound VAC placed and going back tomorrow to reexamine wound and may close it or re-VAC one more time. Fixator remains in place.
My plan to revise fixation is in line with your suggestion - plate symphysis and anterior approach to SI joint.
 |
It appears from post-failure CT scan that the path of the more cephalad IS screw may be helpful to place a longer screw to engage opposite illiac wing as an option, or just anterior SI plates. not likely to do this tomorrow as he remains in a fragile clinical situation regarding his pulmonary status, and profound edema/induration around his pelvis/abdomen and thighs.
I tried to balance timing and initial fixation options with the patient's overall clinical picture, local soft tissue status, and incorporated advice of the traumatologists and urologists on our trauma team. I appreciate your comments, criticisms, and continued interest in this case.