



Date: Mon, 29 Nov 2004 15:41:38 -0600
From: Schmeling, Gregory
Subject: S/P SI joint arthrodesis
Patient is a 61 y/o referred with chronic R SIJ pain. Had "fusion" in 1997. R posterior iliac crest harvested. Still has pain on daily basis. On days it is as high as a 9, others it is as low as a 4, but always is present. She also describes occasional pain down the anterior part of her thighs. She has certain activities that aggravate it and certain activities that do not. When discussing things with her, the pain is really mostly directly in the area of the cage placement.She has tried multiple other modalities to achieve some relief including acupuncture, PT, water walking, TENS, magnetic therapy, lotions, ice, and injections. None of these have given her adequate relief. Prior to attempted SI joint fusion, she had an injection in the joint, which seemed to eliminate her symptoms, and after the attempted fusion she had another injection, which seemed to help as well. That is why she thinks she has persistent pain from this joint. Any thoughts?
|
|
|
|
 |
 |
 |
 |
 |
 |
 |
Gregory J. Schmeling
Director, Division of Orthopaedic Trauma
Medical College of Wisconsin
Date: Mon, 29 Nov 2004 22:20:04 -0500
From: Cliff Jones, M.D.
Interesting way of fusing the SI joint! I would have probably tried SI screw or anterior fusion instead. Even though the "fusion" looks good from the cage insertion, mechanically, I do not know how much stability is provided. Have you obtained a bone scan recently to see if corresponding uptake noted? Have you tried a lidoderm patch? Any response from a medrol dose pack? How did you have this "interesting" and "educational" patient end up on your doorstep? A complex problem in which even if joint is truly stable and fused, she may always have "problems" that surgery and PT may never remove.
Cliff Jones
Date: Tue, 30 Nov 2004 07:01:49 -0600
From: Gregory J Schmeling
This came to me by way of my spine surgeon. I am not sure how he got it. I do not have a bone scan but expect it will be hot. He pain has been ongoing for at least 7 years. I do not know if she has tried the lidoderm or medrol. Maybe worth trying.
Greg
Date: Mon, 29 Nov 2004 23:01:27 -0600
From: Andrew H. Schmidt
Hi Greg,
Have you done single-leg stance AP views of the pelvis? Templeman taught me this and we have seen several similar cases where one finds 2-3 cm of vertical displacement of the hemipelvis.
Andy
Date: Tue, 30 Nov 2004 07:00:02 -0600
From: Gregory J Schmeling
Do not have this film. Will get at next visit. Thanks for the idea.
Greg
Date: Tue, 30 Nov 2004 07:50:12 -0500
From: James Carr
These cases wind up on our doorstep because we fix real SI pathology with real implants. I must say I gave up this operation because I never made anyone better (except displaced posttraumatic). They all come with pain relief from an injection. They may or may not have a positive bone scan. I have tried the Smith-Peterson approach (transgluteal, window the crest, scrape/graft the joint), the anterior approach, and the posterior approach. There is a surgeon in Denver who reports good results with the Smith-Peterson technique. I am not sure what the pain generators are, but I have proven it isn't the SI joint on multiple occasions. If you do decide to fuse it, I would use the Smith-Peterson approach augmented with a sacral screw.
Jim
James B. Carr, MD
Premier Orthopedic Specialists
Columbia, SC 29203
Date: Tue, 30 Nov 2004 07:02:44 -0600
From: Gregory J Schmeling
Thanks Jim.
Greg
Date: Tue, 30 Nov 2004 20:22:22 -0600
From: David Templeman
Greg,
tough case.
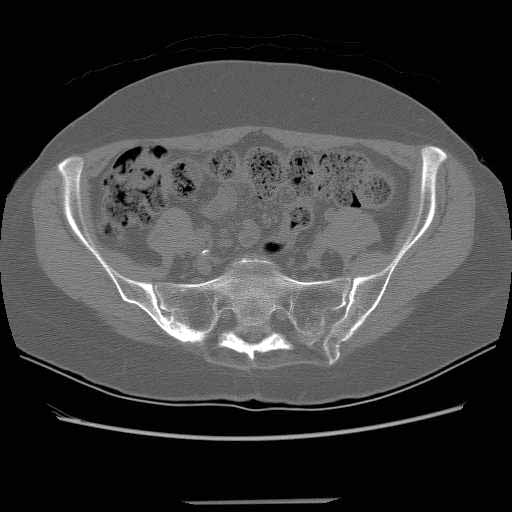
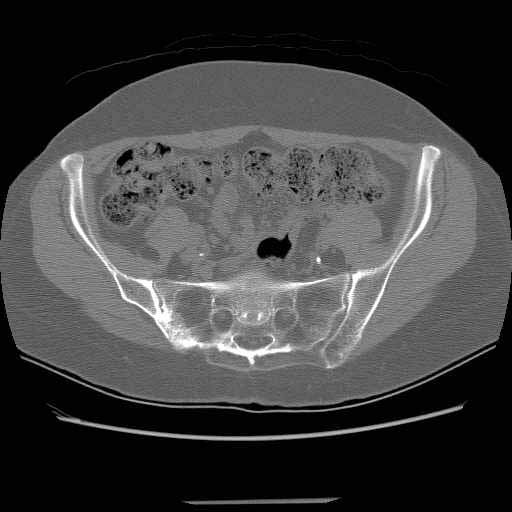
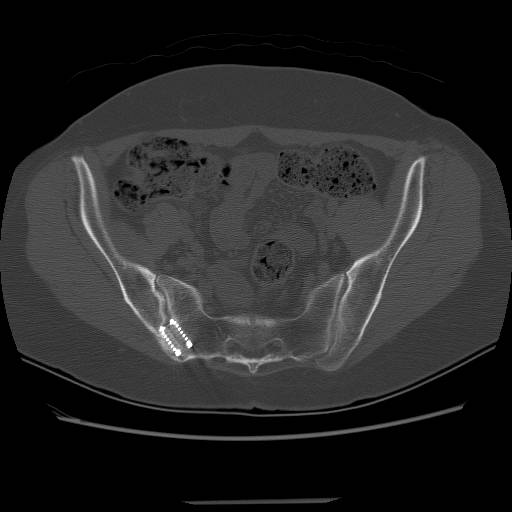
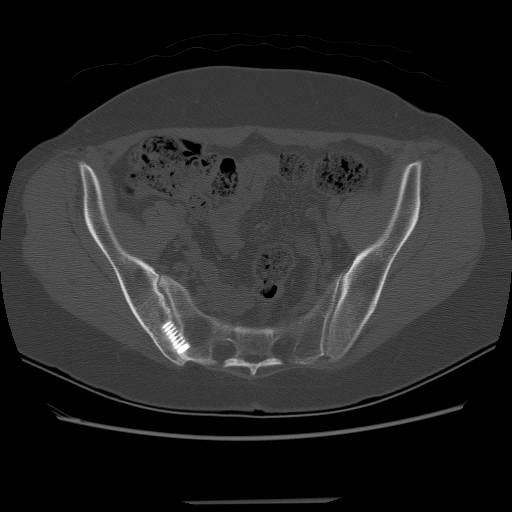
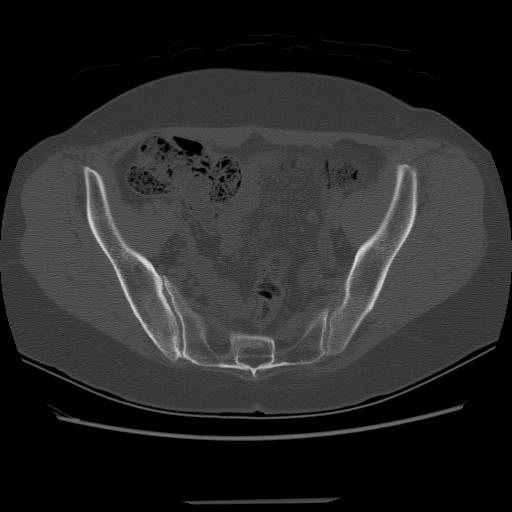
I have seen a couple of patients with the BAK used for SI fusions, they were not helped at all.
there do not appear to be any stress fractures of the iliac wing related to the bone graft on these images.
The CT shows a solid bone mass but the true articular part of the joint remains. This may be a red herring.
The following exams have been helpful for me:
with the patient standing palpate the regions of the lumbar spine and SI joints, when this soft tissue exam reproduces the symptomatic pain I think it is unlikely that surgery will help. Single leg hopping should load the SI joint and reproduce mechanical instability of the SI joint, again without any pain instability of the joint seems questionable.
I completely agree with Jim Carr that we have a poor understanding of the pain generators, I have seen quite a few patients with SI injections and successful fusions who have continued pain.
I would have the patient seen in a pain clinic as a start.
dave templeman