{kind=link}


Date: Mon, 14 Apr 2003 17:08:39 -0500
Subject: Low Acetabular Fx
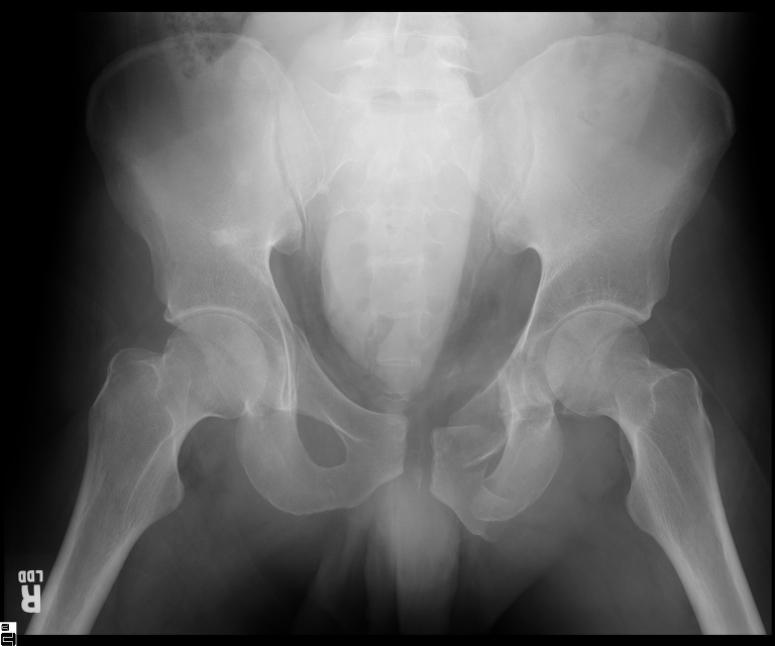
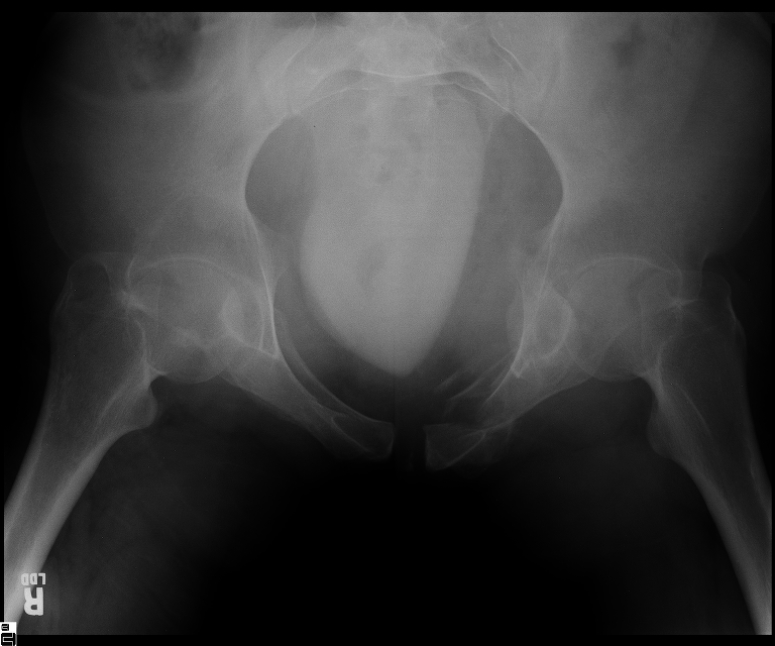
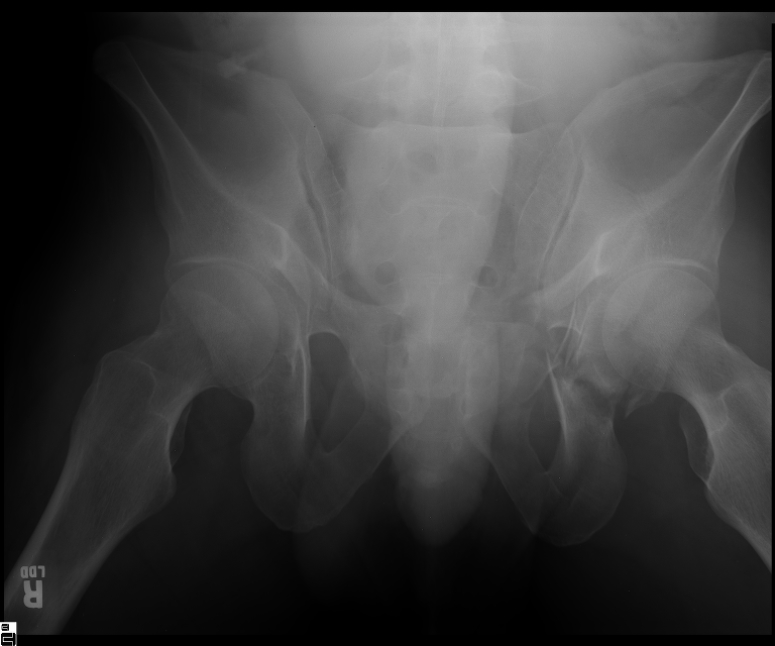
25 yo brittle diabetic, became hypoglycemic and passed out on his motorcycle. Sustained bilateral lateral Hoffa fractures with associated LCL injury on the right and right distal radius fracture. I have questions regarding his pelvic ring/acetabular fracture on the left. Appears to be a very low posterior column fracture with associated posterior wall, marginal impaction. Superior and inferior rami fractures as well on the left giving him a floating segment of inf ramus/ischium/posterior column, but no detectable posterior ring injury. Should the posterior column/posterior wall fracture be addressed surgically because of the marginal impaction? Or is this fracture low enough to be treated non-operatively? I appreciate the input.
|
|
|
|
|
 |
Marcus F. Sciadini, M.D.
Assistant Professor,
Dept. of Orthopaedics & Rehabilitation
Vanderbilt University School of Medicine Nashville
Date: Mon, 14 Apr 2003 22:14:46 -0500
From: Frederic B. Wilson, M.D.
Marcus,
I believe the more serious component of the acetabular fracture to be the large (almost 50%) impacted, comminuted zone of the posterior wall. In several series, including the one I reported at the AAOS in 2002 in Dallas of 100 acetabular fractures with posterior wall involvement, all repaired by a single surgeon (Kyle Dickson), those with posterior wall impaction did significantly worse than those without. Nevertheless, the large area of involvement, as well as a joint designed for very low tolerances of "out of round", would indicate that the best chance for avoiding early degenerative changes would be an anatomic repair.
Dr. Darby Webb is updating Kyle's results in a series well over 100 acetabular fracture with posterior wall involvement (whether simple or associated types) that continues to show that impaction is a serious detriment to outcome, regardless of the fracture pattern.
Fred Wilson
Tulane Orthopaedics
Date: Tue, 15 Apr 2003 07:41:50 -0500
From: Adam J. Starr, M.D.
Hi Marcus.
It's an interesting case. The plain films show the impaction, but most of the joint looks pretty good. The CT cuts look awful, though.
I think I'd fix it, but I think it'll be hard to get the impaction piece to stay put. Everybody uses bone graft and screws - but everybody has bad results from these, too. So I guess the bone graft and screws aren't so hot?
The impaction is so big I don't think I would ignore it. It IS down low, but it takes up almost the whole southern hemisphere of his joint.
The fact that he's a motorcycle-riding, brittle diabetic who passes out from hypoglycemia makes me worry about the risks of non-compliance, though. I'd have a long talk with him about what I was trying to achieve with his joint, so he'd know what I expected.
Good luck.
Adam Starr
Dallas, Texas
Date: Tue, 15 Apr 2003 11:44:26 -0700
From: Chip Routt
Marcus-
Here's a thought regarding your patient...you work with a very bright and experienced acetabular surgeon...show the films to Phil Kregor and do whatever he advises.
Regarding Adam's comments-"Everybody uses bone graft and screws - but everybody has bad results from these, too. So I guess the bone graft and screws aren't so hot?"
Whoa pardner!
I disagree with Adam's broad statement. The surgeon must elevate impaction, reduce it accurately, and support it...then, success with impaction is anticipated.
There are different types of acetabular impaction injuries...some(few-usually very high energy injury mechanisms) are wide zones of crush-cartilage/subchondral/cancellous-extremely small comminuted bits which exude with the fracture hematoma during the exposure.
Others(most) are discrete osteochondral fragments which can be elevated/reduced/stabilized...these very different acetabular impaction injury types should not be lumped together regarding treatment & prognosis.
PLEASE PLEASE PLEASE don't have a fatalistic approach to acetabular impaction...most can be easily treated and they are vital to good results.
Be aware of, and be patient with, these important fragments.
Work hard to plan preop, elevate, reduce, and support these fragments whenever possible...remember that postop CT scans are very helpful to assess your work and help you technically improve regarding their reductions and support techniques.
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
325 Ninth Avenue
Seattle, WA 98104-2499
Date: Tue, 15 Apr 2003 13:55:58 -0500
From: Frederic B. Wilson, M.D.
Chip,
Great advice! Both with respect to Phil and with respect to being fatalistic about impaction. We make every attempt to make these anatomic, recognizing that we probably have only one best chance to do it. My comments were only intended to convey the experiences of several people that have shown that impaction is tough to get perfect and correlates with somewhat worse results. To me that is important in my pre-operative interview with the patient and family in terms of expectations.
Frederic B. Wilson, M.D.
Assistant Professor
Trauma and Adult Reconstruction
Department of Orthopaedic Surgery
Tulane University School of Medicine
New Orleans, LA, 70112
Date: Tue, 15 Apr 2003 15:28:23 EDT
From: Tadabq
At least be realistic if not fatalistic.
TD
Date: Tue, 15 Apr 2003 16:04:13 -0500
From: Sciadini, Marcus
Thanks to all for the input. I agree that marginal impaction fragments, particularly large ones, are amenable to elevation, anatomic reduction and fixation with not necessarily dismal results. My own thoughts in this particular case are that even though this fracture is situated in a fairly inferior position, the resultant increased acetabular volume may negatively impact his joint mechanics. I'llsend the post-op images for critique.
Respectfully,
Marcus F. Sciadini, M.D.
Date: Fri, 18 Apr 2003 08:44:50 -0500
From: Kyle Dickson, MD
dear marcus,
interesting case. I believe a common mistake is saying that the dome is ok so I can treat this nonoperatively. This only works for tr and t type fractures not posterior column posterior wall fractures. Matta's results show no difference with impaction. Mine show worse results with impaction but still better results than nonoperatively. The really bad ones are the elderly with dome impaction but I ve been surprised by a few of those as well. This I more posterior and I think will do well with good fixation. This means a good reefing behind the piece (?2.7mm or 2.0mm to get more screws) to prevent the late collapse. I also am very gingerly with their post op tdwb x 3 months with no pt to that extremity. Hope this helps.
PS: was that your video of impaction correction and can I use it in talks?
Thanks kyle
Date: Fri, 18 Apr 2003 14:27:25 -0500
From: Sciadini, Marcus
Dr. Dickson:
Thank you for the feedback! I have yet to be able to fix this young man's acetabulum because he has developed significant pulmonary problems, but will certainly let you know how it turns out. Regarding the video, not sure what you're referring to, but I don't have a video of impaction elevation (wish I did!).
Marcus
Date: Fri, 18 Apr 2003 19:28:40 -0400
From: Bill Burman
Kyle, Marcus
I took the liberty of linking an animated gif to the mention of marginal impaction of the posterior wall. These can now be directly imported into Powerpoint. It was created from the graphics of Bob Brumback and the JOT. They own it.
Date: Sat, 19 Apr 2003 13:23:31 -0400
From: James Carr
One set I find useful for large impacted pieces is the minifragment set with extra long screws. They are great for holding the fragment into place, and facilitate other steps like bonegraft, and repairing the wall itself. Drives my hand guys nuts when I take their set for this!
Date: Wed, 23 Apr 2003 14:46:46 -0500
From: Sciadini, Marcus
Here are the immediate post-op results of my case. Standard Kocher-Langenbeck posterior approach to the acetabulum, encountered extensive comminution of the inferior posterior column, postero-inferior subluxation of the femoral head, multiple marginal impaction fragments. Fixed with multiple 2.7 and 2.0mm lag screws, a 2.0mm mini-frag plate, 3.5mm recon plate, and 2.7 mm recon plate. Bone graft for support of marginal impaction harvested from greater trochanter.
 |
 |
 |
 |
Marcus F. Sciadini, M.D
Date: Thu, 24 Apr 2003 09:28:08 -0500
From: Kyle Dickson, MD
Looks good the only comment is I would bend your more lateral plate laterally instead of medially to contour the posterior column better. Are you planning to get a ct?
kyle
Date: Thu, 24 Apr 2003 13:15:07 -0500
From: Sciadini, Marcus
The ct scan cuts are, I believe, on the same website as the plain films...
MFS
Date: Thu, 24 Apr 2003 20:13:03 -0500
From: Kyle Dickson, MD
Sorry found them. Tough fracture - it looks like there is still some impaction and the posterior column is still internally rotated around the head. What do you think about your reduction?
kyle
Date: Sat, 26 Apr 2003 21:47 EST
From: Bill Burman
Kyle
You say "there is still some impaction and the posterior column is still internally rotated around the head."
I wonder if you could select and download the appropriate CT cuts (right click on the image on PC; sustained click on the image on Mac) and draw some arrows and lines where you have concerns. If you then attach these "marked-up" images to e-mail, I'll append them to the web page so that it can help folks (such as myself) who are not readily seeing these deformities - so we can better recognize them.
As shown with lines drawn along the iliac crests and quadrilateral surfaces in your OTA BFC talk on "Associated Pelvic Injuries", are there any references which provide normal values and correlation with outcome?
I would also like to request a drawing which would show optimal contouring and positioning of the lateral posterior column plate.
Thanks for your help in increasing the educational value of this case.
Bill