


Date: Fri, 3 Sep 1999 18:53:12 +0300
Subject: multi trauma
Dear All,
Attached here few x-rays of a multi-trauma patient. He is a 51years old man,sustain MVA at 08/15/99 and refer to our hospital few days ago, more than twoweeks after injury. He sustain Bilateral femoral fracture including femoralneck, A right humerus fracture, right distal radius fx, left open ulnar fx,right tibial plateau (type III) fx and Chopart fracture dislocation of the rightfoot. At the other hospital where he was admitted, He underwent laparotomy andfixation of both femur by reconstruction IMN, application of Ex Fix to thehumerus, and reduction and K.W. fixation of the Rt foot. He is currently stable and conscious. He is scheduled next week for replacing of the Rt IMN to aretrograde nail and pinning (6.5 mm screws) of the neck fracture, fixation ofthe ulna, distal radius and tibial plateau.
We are seeking for ideas about the left femur: either tore-operate or leave it as is, and if to operate - what approach.
Thank you - Nachshon Shazar, Orthopaedic Trauma Service, Sheba MedicalCenter, Tel aviv, Israel.
| | |
Date: Sat, 4 Sep 1999 13:01:14 +0300
From: Anton V. Vakulenko
Dear Sir
I suggest that re-osteosynthesis is not needed because of good fixation ofthe left femur fragments. Central fragment of the left femur after sometime will assimilate to the host bone due to callus formation. Attempts tofix central fragment will due to it's devitalisation. Intensive reparativetreatment with administration of calcium and improving microcirculationdrugs are highly recommended.
Sincerely - Anton V. Vakulenko
Date: Sun, 05 Sep 1999 22:28:40 EEST
From: Mehmet Arazi
Dear Dr. Shazar
The implant selection was right but application technique and length of the nail were not. Lateral x-rays of the hip should be taken to confirm reduction of the femoral neck (bilaterally?).
In my opinion both fractures sould be revised with closed interlocking nailing with the same nail, appropriate length using two proximal locking screws to the head. Two screws for distal locking must be also used because these are very unstable fractures.
Supine position for nailing more suitable than lateral. We use routine reamed nailing. It is your choice.
Best luck - Mehmet Arazi, MD, Konya, Turkey
Date: Mon, 06 Sep 1999 15:17 EST
From: Bill Burman
I have written to Nachshon Shazar about this case off-list so my apologies to himfor redundancy. I realize since I don't operate I should shut-up and notback-seat drive but this list is dull right now and the salvage of failed recon nails is areal problem - so I will do my best to provoke.
I would probably start out with a fluoroscopic evaluation of the stability of thefixation. If it was grossly unstable, I would think that at least the neckfracture needs better reduction and fixation - but there appears to be nothingleft on the lateral side to hold a side-plate or screws needed for neck fixationwithout a proper interfragmentary reconstruction of the proximal femur and thenthat would mean - even with indirect reduction - a big exposure and a big plate.
 |  |
In the 80's, I spent some time in the UK. They had no interlocking nails then andI found a Huckstep nailing kit in the OR closet. (Huckstep-RL Clin-Orthop. 1987Nov(224): 12-25)
 | 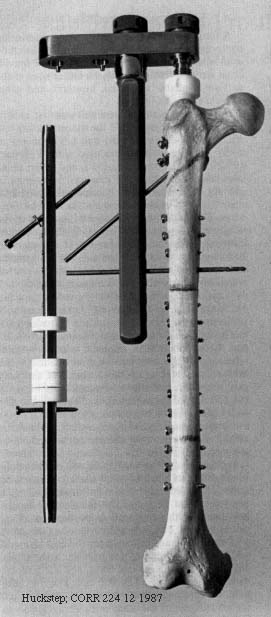 |
It has transverse locking screw holes every 2 cm and oblique screw holes at thetop for neck fixation and so it is like a big intramedullary plate. The externaltargeting jig for the screw holes was very rigid and I was able to interlock in aclosed manner. The only problem is that it was a straight, large diameter (12.5mm) device which could comminute a proximal femur (which has already been done inthis case). The other problem was that it was uncannulated so getting it acrossthe various fractures closed without a guide wire can be tricky.
At any rate, if a device like this is available to you, it may be worthconsidering. After a provisional cerclage/reduction of the proximal femoralshaft, you could get good fixation on at least the proximal medial cortex withmultiple locking screws. You could get perhaps 2 screws into the headneck-fragment through the nail and maybe one or two lag screws or Knowles pinsaround the nail.
If there is delayed union of the neck after the shaft heals, I would remove thenail and do a valgus intertrochanteric osteotomy with a dynamic compression screwor angled blade plate as described in the references below.
Bill
Marti RK, Schuller HM, Raaymakers EL; Intertrochanteric osteotomy for non-unionof the femoral neck.; J Bone Joint Surg [Br] 1989 Nov;71(5):782-7
Huang CH; Treatment of neglected femoral neck fractures in young adults.; ClinOrthop 1986 May;(206):117-26
Lifeso R, Younge D; The neglected hip fracture.; J Orthop Trauma 1990;4(3):287-92
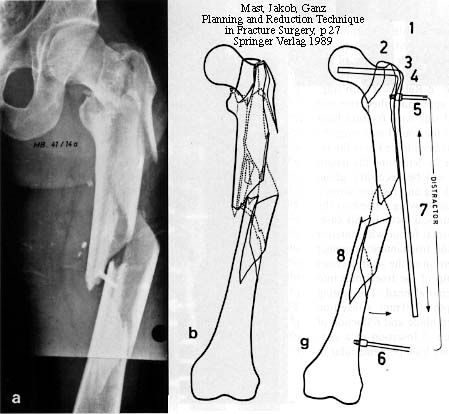
Ballmer FT, Ballmer PM, Mast JW, Ganz R; Results of repositioning osteotomies indelayed healing or pseudarthrosis of the proximal femur; Unfallchirurg 1992Oct;95(10):511-7
From: Nachshon Shazar
Date: Thu, 16 Sep 1999 14:43:24 +0200
We fluoroscoped every thing in the OR under anesthesia. It was clear that the Ltproximal side is unstable, in mal-position and the nail is probably outproximally.
On the Rt side, the proximal construct was stable but the distal (the shaft fx)was not.
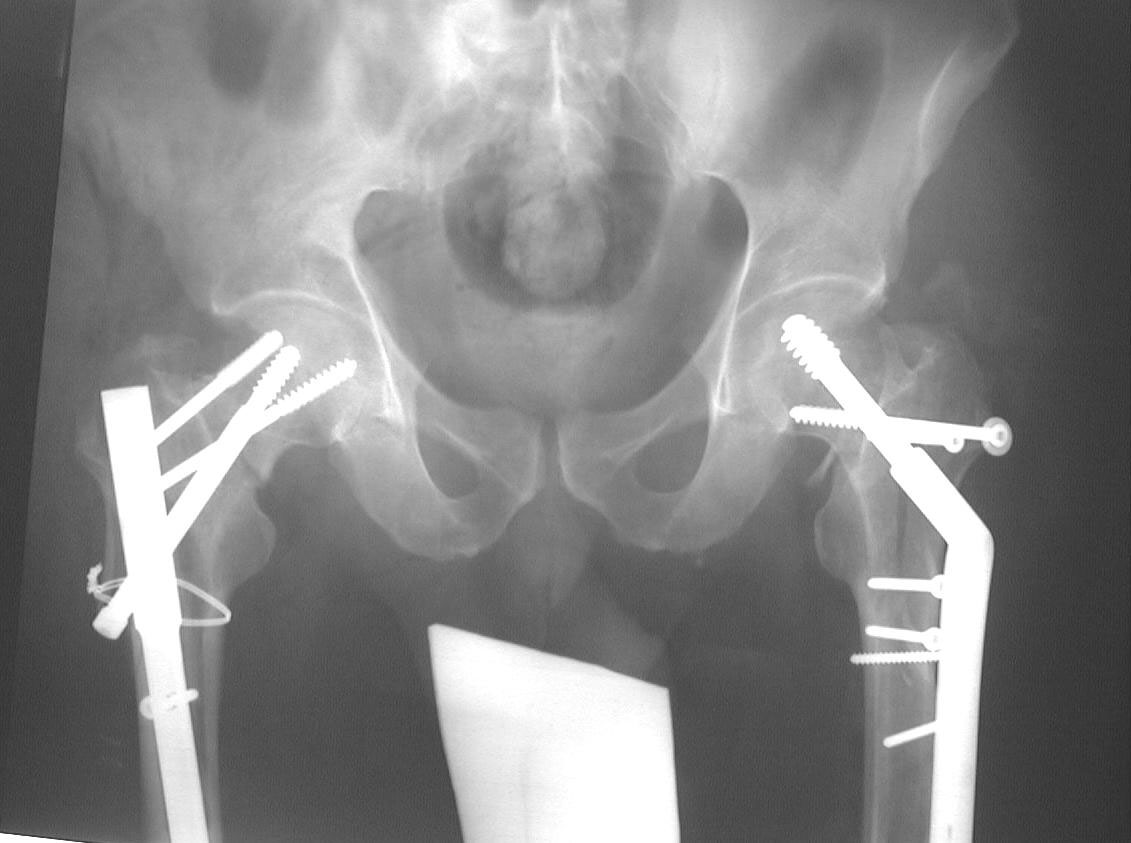 |  |  |  |  |  |
We decided to fix the Lt femur with a few lag screws on the proximal part andstabilize the femur with long Richard plate that was inserted in a sub-muscularfashion, in order to avoid opening the main shaft fx (the so-called biologicfixation - see Lt leg incisions.).
On the Rt side I replaced the recon nail with a longer one (accepting its toolateral and anterior entering point), I added a proximal locking screw (anterior toposterior) in the subtrochanteric region through a self-made extra hole, and two 6.5cancellous hip screws posterior to the nail.
Nachshon Shazar, Orthopaedic Trauma Service, Sheba MedicalCenter, Tel aviv, Israel.