

Date: Tue, 4 Nov 2003 21:19:37 +0545
Subject: Shaft Humerus Fracture with Nerve Palsy
From: Dr. M. P. Shrivastava
Dear all,
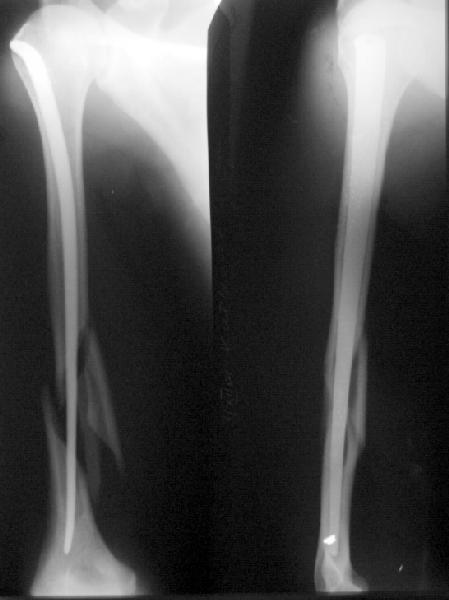
Kindly give your valuable opinions regarding the treatment of a closed type of comminuted fracture of shaft of the left humerus with radial nerve palsy ( wrist drop) in a 21 years young male patient . The patient sustained fracture due to RTA two days ago. Images are attached herewith.
| |
Dr. M. P. Shrivastava
Consultant Orthopaedic Surgeon
Nepal Medical
College Teaching Hospital
Jorpati, Kathmandu, Nepal
Date: Tue, 4 Nov 2003 17:12:28 -0800
From: Steve Groman
Assuming that this is a closed injury and that there was no penetrating injury, and If you can achieve alignment by closed means, I would do so, and wait expectantly, as the vast majority of these radial nerve palsies will return spontaneously. If the radial nerve was intact, and then the fracture manipulated and THEN the radial nerve went out, I would recommend exploration and ORIF of the humerus.
Date: Tue, 4 Nov 2003 21:48:12 EST
From: Aobonedoc
Hello:
I would try closed treatment first. However, fracture appears unstable and looks like it will fall into varus. Retrograde flexible nails (ie Rush Rods) would be a minimal procedure that could supplement functional bracing. I would try not to nail antegrade so as not to injury the rotator cuff. There are some nails that you can use that will not violate the cuff. I do not think I would choose ORIF. If you do, you can look at the nerve. I think one can safely watch the nerve for 3 to 6 months if it was out from the original injury. Good luck.
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and
Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005
Date: Wed, 5 Nov 2003 07:42:50 -0500
From: James Carr
He will do well in a light weight hanging arm cast. The reduction will improve over the first few weeks in that device. Don't jump to operative treatment for arbitrary alignment numbers- this fracture will heal well even if not in perfect apposition. If it is in varus persistently, just place a small pillow in-between the patient and the cast- this can be ace wrapped to the cast if necessary. The nerve will take typically 4 months to return, but sometimes as long as 6. Functional outcome is good in my estimation, despite the dramatic appearance of the x-rays.
Jim Carr
Date: Wed, 5 Nov 2003 16:00:59 -0700
From: Terry Finlayson
I would ORIF with a 4.5mm DC plate placed anteriorly on the humerus through an anterolateral (Henry) approach. This would provide anatomic alignment, rigid fixation to allow immediate ROM of shoulder and elbow and would provide direct visualization of the radial nerve. I would be concerned that closed treatment of this fracture would put the nerve at risk for ongoing trauma.
Terry I. Finlayson, MD
Alpine Orthopaedic Specialists
Logan, UT
Date: Sat, 8 Nov 2003 14:00:44 +0500
From: Alexander Chelnokov Hello Dr.,
DMPS> Kindly give your valuable opinions regarding the treatment of a closed type of comminuted fracture of shaft of the left humerus with radial nerve palsy ( wrist drop) in a 21 years young male patient .
We routinely perform antegrade closed nailing. In the case no matter what particular implant and technique is used. No need of nerve revision - virtually all radial nerves in closed fractures proceed to spontaneous recovery.
Best regards,
Alexander N. Chelnokov
Ural Scientific Research Institute
of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Sun, 9 Nov 2003 21:17:10 +0545
From: Dr. M. P. Shrivastava
Dear Dr,
We routinely perform antegrade closed nailing.
Do you do static locking as well while going for antegrade nailing?.
Dr. M. P. Shrivastava
Kathmandu, Nepal
Date: Sun, 9 Nov 2003 21:20:38 +0500
From: Alexander Chelnokov
Hello Dr.
DMPS> Do you do static locking as well while going for antegrade nailing?.
At the humerus we use flat titanium nails without screws.
Best regards,
Alexander N. Chelnokov
Ural Scientific Research Institute
of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Mon, 10 Nov 2003 21:45:51 +0545
From: Dr. M. P. Shrivastava
Dear Dr.
We have doing solid humeral nailing either antegrade or retrograde with static locking all the time. I would be happy if you could send me few pictures of humeral fractures treated with flat nailing. I am attaching few images.
 |
Dr. M. P. Shrivastava
Kathmandu, Nepal
Date: Mon, 10 Nov 2003 21:44:39 +0500
From: Alexander Chelnokov
Hello Dr.,
DMPS> static locking all the time. I would be happy if you could send me few pictures of humeral fractures treated with flat nailing.
THX, nice images.
I attached a similar example - postop and 4 month.
 |
 |
Best regards,
Alexander N. Chelnokov
Ural Scientific Research Institute
of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Mon, 10 Nov 2003 18:31:48 EST
From: Tadabq
Alex,
Can you provide some additional information on the "flat" nail for the humerus shaft. That is a great case you posted. Is it made of titanium? It looks to be tapered with larger diameter or width proximally than distally. What is the cross sectional shape? Who makes it? It seems similar but different (and perhaps better for humerus shaft indication) from our Ender pins or AO flexible nails.
Tom DeCoster
Date: Thu, 13 Nov 2003 00:03:42 +0500
From: Alexander Chelnokov
Hello Tadabq,
TAC> humerus shaft. That is a great case you posted. Is it made of titanium?
Yes. The family of nails (for all long bones) was developed in Yaroslavl, Russia, in late 80s, some bibliography is below.
TAC> It looks to be tapered with larger diameter or width proximally than distally.
Yes. For the humerus in lateral view it is narrowing from top to bottom to fit the medullary canal without reaming.
TAC> What is the cross sectional shape?
Rectangular. Thick is 3 or 4 mm for humerus.
TAC> Who makes it?
The strong and weak point of the technique is that each nail must be individually customized. Some manufacturers in Russia make "prototypes" for the nails which are to be completed by end user-surgeon to fit standard lateral view of the contrlateral humerus. We have a small workshop in our institution where the nail can be prepared using vice, hammer, saw, emery etc. I suppose this feature prevents wide dissemination of the technique. We use them with some modifications for forearm and humerus and still have not enough motivation to migrate to modern industrial type locked nails. It is cheap and effective.
TAC> It seems similar but different (and perhaps better for humerus shaft indication) from our Ender pins or AO flexible nails.
I don't think comparative study was ever performed. The rectangular shape provides rigidity in sagittal plane and elasticity in frontal. Though the techique is not fool-proof, requires skills because the nail can be made wider than the canal is, or longer than necessary which results in the OR with search of bailout.
Best regards,
Alexander N. Chelnokov
Ural Scientific Research Institute
of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
--------------
Functional intraosseous osteosynthesis of diaphyseal fractures of long bones]
The analysis of the treatment of diaphyseal fractures of tre long bones with functional intraosseous osteosynthesis (FIO) of 593 patients (675 bones) during three years is presented. The techniques of osteosynthesis have been worked out by the author and are performed without using an electro-optical transducer and drilling out of the medullary canal. At the postoperative period no immobilization with a plaster cast is necessary. The function of the operated extremity is restored before the fraction is consolidated. The disability terms are shorter than usual. There have been no non-unions, false joints or contractures. There was one case of osteomyelitis (0.1%). The definition of FIO is given, the conditions for its performance and the requirements for the intraosseous fixator are presented as well as the facts of making use of FIO in the treatment of non-unions and false joints of the long bones are listed.
[Intraosseous osteosynthesis of closed diaphyseal fractures of the forearm bones]
The author has proposed a method of intraosseous osteosynthesis in closed diaphyseal fractures of the bones of the forearm according to a closed or half-open technique using a specially prepared titan alloy BT6 rod. After the operation no immobilization by plaster bandage is necessary. The function of the extremity is restored long before the consolidation of the fragments is achieved. The period of disability after the operation is shorter than after the traditional methods of treatment.
[Treatment of diaphyseal fractures of long tubular bones by functional intraosseous osteosynthesis]
A clinical analysis of treatment of 328 diaphyseal fractures of long bones in 304 patients by functional intraosseous osteosynthesis which is not to be followed by plaster immobilization has shown that the function was reestablished long before the consolidation. The functional intraosseous synthesis was performed without drilling of the bone marrow cavity, without special appliances or devices. Terms of invalidism are shorter than traditional ones. Consolidation of the fractures takes place within 5-10 months. The nails are removed at the same terms. The method is of low cost, easy in use, reliable, is followed by few complications.
Date: Wed, 12 Nov 2003 17:46:46 EST
From: Tadabq
Alex
Thanks for the informative response about details of the "flat" nail. I'm still unclear about the geometry of the nail. It is rectangular in cross section with a thickness of 3 or 4 mm. What is the width (or the length of the other side of the rectangle)? This is a tapered nail (wider proximally than distally). What is the proximal width and what is the distal width? Is this part of the customization so that each nail is different? If so, what were the proximal and distal widths of the nail in the case you showed, or a typical nail?
The length is custom made for each patient?
How do you hold on to the nailto put it in and take it out?
Thanks. Very interesting and potentially useful implant.
Tom DeCoster
Date: Thu, 13 Nov 2003 20:45:03 +0500
From: Alexander Chelnokov
Hello Tadabq,
TAC> section with a thickness of 3 or 4 mm. What is the width (or the length of the other side of the rectangle)? This is a tapered nail (wider proximally than distally). What is the proximal width and what is the distal width?
I attached an example.
 |
The the distal end of the prototype is 3 or 4 mm, wide end - 18 or 20 mm. One can cut any part of the workpiece.
TAC> Is this part of the customization so that each nail is different?
In general yes.
TAC> If so, what were the proximal and distal widths of the nail in the case you showed, or a typical nail?
About 14 mm and 4 mm.
TAC> The length is custom made for each patient?
Exactly.
TAC> How do you hold on to the nail to put it in and take it out?
It is inserted by hammering, last centimeters using a pushing bar with a notch. To take it out one can use plier or forceps (conventional approach), recent years we drill 1-3 holes (5 mm), which allow to use either hook or wire loop connected to a sliding hammer. Also through the holes we can insert locking screws which can be useful in case of upper third fractures with wide and short proximal fragment.
Best regards,
Alexander N. Chelnokov
Ural Scientific Research Institute
of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia