



Date: Thu, 08 Feb 2001 18:40:27 -0500
From: Michael Sirkin
Subject: Infected tibia nonunion
This is a 45 year old gentleman who 8 years ago sustained a midshaft tibia fracture originally treated with plate and screws which became infected. The plate and screws were removed, dead bone was resected and Ilizarov was placed with proximal corticotomy and transport into distal defect. Multiple complications during this including refracture and infection.
|
|
|
|
He now shows up in my clinic with pain and deformity as seen in the images. He has a draining sinus which drains on and off intermittently. He really wants to save his leg but i think an amputation will serve him best. He has a rigid ankle and midfoot. Currently his ankle is fixed in about 10 degrees of dorsiflexion. He ambulates with crutches because of his pain. He has sensation distally with good capillary refill, no palpable pulse. Angiogram shows all 3 vessels present in leg.
How many think he should have an amputation and how many would try reresection, flap and transport.
Date: Fri, 9 Feb 2001 05:12:12 -0800
From: bruce meinhard
Michael,
I would give it one more shot to gain a well aligned leg. This might require a soft tissue release at the ankle or an arthrodesis as a secondary procedure. First a soft tisue procedure like a flap to bring in quality tissue and at 4-6 weeks after that another ilizarov and corticotomy to correct the deformity more gradually. The foot could also be included to correct its deformity at the same time, or the ankle and foot could be taken care of at a later date. This would only mildly prolong his treatment phase.I would like to hear from our Russian Friend and correspondent Alex as well on this. Looking forward to seeing you again at your lecture this month at Stony Brook
BPM
Date: Fri, 9 Feb 2001 11:11:07 -0000
From: Nuno Craveiro Lopes
Michael,
In spite of infection this is a hypertrophic pseudarthrosis so it will consolidate and the infection "will burn out on the fire of the regenerate" as Ilizarov used to say. So I advise you to use a Ilizarov frame again to do simultaneous axial correction and if necessary, lengthening without any surgical approach to the lesion. I attach a sketch of the proposed frame and a clinical case.
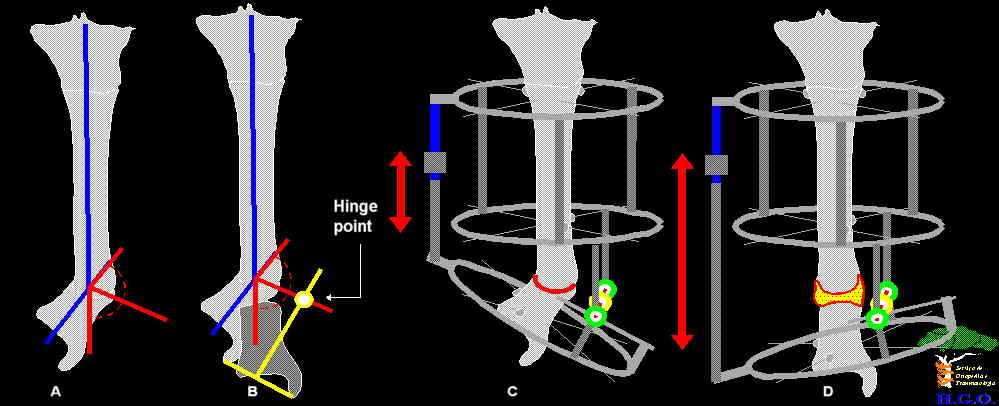 |
| A,B) Finding the hinge point. C) Frame assembly. D) Correction.� |
 |
| A) Pre-op: Infected hypertrophic pseudarthrosis.
B) Frame assembly at the beginning of correction. C) Frame assembly at the end of correction. 5 months in frame. D) Final result. |
Best regards
Date: Fri, 9 Feb 2001 19:25:35 +0500
From: Alexander Chelnokov
Hello bruce,
bm> I would give it one more shot to gain a well aligned leg. This might require [...] phase. I would like to hear from our Russian Friend and correspondent Alex as
I can't be silent observer after this :-)
Well, I hardly ever can express an opinion about amputatate or not - it is beyond my experience and requires knowledge of circumstances, specific for local population, like availability of prostheses, costs, social guarantees, expected quality of life, typical patient satisfaction and so on.
So i only comment the second option. I would agree with you and Dr Lopes in general that Ilizarov-based techique can be applied in this case with good chance of success. Though I wouldn't be so optimistic about that infection will definitely "burn in the fire" - but maybe it will become more localized while ends are healing at some part of the bone diameter. So anyway i would start with closed frame assembly, hinges according to the real plane of the deformation and gradual axial correction. I would also attempt to stir up his ankle using slight distraction and hinges, at least to place the foot to more functionally acceptable position (BTW how about 1st phalango-metatarsal joint?).
Further activity will depend on results of the procedure. Maybe it will be definitive one, maybe he will proceed with sequester removal, or partial or segmental resection+transport... Good luck anyway! Keep us informed.
Best regards,
Date: Fri, 09 Feb 2001 08:49:42 -0600
From: Adam Starr
I would vote for amputation with debridement of all infected tissues.
Date: Fri, 9 Feb 2001 10:20:14 -0700
From: John Ruth
BKA seems most appropriate. He needs to get on with his life!
John Ruth
Date: Fri, 09 Feb 2001 15:18:57 -0500
From: William Obremsky
Michael,
I would vote for a BKA.Ę If patient was amenable and able to tolerate it, I think an Ilizarov would be your only surgical option.
Bill Obremskey
Date: Fri, 09 Feb 2001 15:04:48 -0600
From: Steven Rabin
he's already had one try at the Ilizarov type procedure without success and multiple complications. Unless you know that the Ilizarov procedure and followup was done poorly, I would suggest that its time for the BKA. It has the least chance of failure, and most chance of finally some return to painless function. If you review old records or talk to the original surgeon, and the previous transport violated basic principles or was done poorly, and you truly believe you can do a better job than the previous guy, then you could consider another Ilizarov, but I think this should be the last try.
Date: Fri, 9 Feb 2001 14:08:29 -0600
From: Anglen, Jeffrey
8 years?! He should have had an amputation about 5 years ago. If it was me I would have.
Jeff
Date: Fri, 09 Feb 2001 15:18:56 -0500
From: David Dr. Sanders
rigid ankle and midfoot => amputation
-dave sanders
Date: Fri, 9 Feb 2001 21:13:59 EST
From: Roy Sanders, MD
He probably would do better with an amp, but otherwise he would need to have his canal opened and reamed multiple time, which would give you a problem with the skin because the tissue, is bad. This means he would need epigard coverage while you do this, because straightening him out will probably require open osteotomies which then will prevent wound closure. Then he will need a flap at 5-7 days, then a nail, and 6 weeks of culture specific antibiotics. this may work to get him healed and straight he will probably require multiple debridements in the future but ultimately will calm down. Then the problem will be his foot and ankle, but that will be another reconstruction. But hey, I thought that lizard rod stuff was easy, and worked all the time. What gives?
Roy Sanders, MD, Tampa, Florida