


Date: Tue, 1 Oct 2002 09:57:12 -0700
Subject: Pelvic Fx - Open APC3/Polytrauma
I am presenting this case for opinion of list members.
33-year-old male. Motorcycle vs. Auto. Injuries included:
Hemodynamically unstable on presentation with systolic pressures in the 70's Mean arterial pressure 45-50. Brisk bleeding from open wound. C-Clamp placed emergently in ED, open wound packed. Then to angio for embolization of SGA . Then to OR for formal washout of open wound, diverting colostomy.
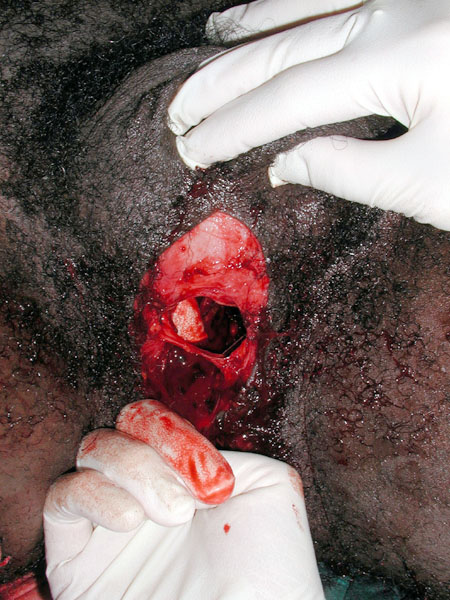
Pt is now 5 days out with C-Clamp in place. Other skeletal injuries have been treated with ORIF. Pt is stable, small L sided pulmonary infiltrate but no fevers and a clean perineal wound. Pre- and post C-clamp X-rays as well as post clamp CT included. The clinical photo shows the open wound scrotum is above and finger in the anus and out the anterior wall into the open wound.
Questions I need help with:
Thanks for any and all input.
Brian D. Solberg, MD
Director Orthopaedic Trauma Services
Cedars-Sinai Medical Center
Los Angeles, CA 90048
|
|
|
|
 |
 |
 |
 |
Date: Tue, 1 Oct 2002 12:32:03 -0700
From: Zsolt Balogh
1. You saved the life of the patient, now you can fix the symphysis whenever you want if the patient is over the immunological "downhill".
2. Iliosacral screw + sacral bar and/or plate sounds overkill...You can percutaneously fix with IS screw but you need to reconstruct the anterior part of the ring.
Is Dr. Routt lurking?
Congratulation so far!
Zsolt Balogh, MD
Date: Tue, 1 Oct 2002 16:06:42 -0500
From: Adam Starr
Hi Dr Solberg,
At what point can I plate the symphysis? Is there an absolute contra-indication to symphysis plating in open APC fractures like this
I don't think there's an absolute contra-indication, but you still run a risk of infection if you plate the guy's symphysis now. The least risky thing would be to use an anterior ex fix frame. My preference would be to use a symphyseal plate, but you definitely run a risk of pus, so I think I'd be chicken to do it now. I think I would use a supra-acetab ex fix until that wound healed up and then I'd go ahead and plate it.
Is there biomechanical or clinical data to suggest that Ilio-sacral screws augmented with either a transacral plate or bar are superior to screws alone in widely displaced posterior lesions such as this?
We presented our data on perc iliosacral screws for vertically unstable pelvic fractures at the OTA a couple years back, and none of our failures were in SI joint dislocations. The failures were all in the sacral fractures. So, I'd use perc iliosacral screws. I would worry about the Ganz clamp wounds, but I think I'd still go ahead and use the screws.
This is a nice case - the best thing is that you managed to save him, which is tough in this type of patient.
Adam Starr
Dallas, Texas
Date: Thu, 3 Oct 2002 07:50:00 -0700
From: Chip Routt
We assume tetanus, IV antibiotics, open wound I&D, and fecal diversion due to rectal involvement.
The perineal/perirectal open wound debridement is significantly improved using a Pfannenstiel exposure. Using the traumatic wound only for debridement can be inadequate.
Repair the anal sphincter if you can during the initial op.
Don't forget in more extensive perineal wound situations (with similar symphyseal disruption) that you can clamp the disrupted symphysis temporarily through the open wound using a routine pointed reduction clamp...it's quicker/safer/easier than the C-clamp posteriorly...use that wound when you can...it really shuts down wound area hemorrhage.
Symphyseal plating is accomplished after accurate reduction during that I&D procedure, usually on the injury date. Local bleeding halts after symphyseal reduction. It is not contraindicated, but delivers a "surface exposure" to the contaminated area. Be accurate, be quick.
Accurate early symphyseal reduction typically facilitates the SI "realignment"/indirect reduction/whatever you want to call it.
Iliosacral screw fixation of the SI disruption is indicated. The initial screw can be a lag if compression is needed, and the subsequent screw can be fully threaded to "set" the fixation. If the lag is a "spinner" after you've compressed the disruption, then exchange it for a fully threaded screw, after you've "set" the fixation.
Again, I prefer to do all this on the injury date supine...iliosacral screws are "internal unilateral C-clamps".
Accurate C-clamp application is best accomplished in angio under fluoro while the reduction is temporarily maintained with a circumferential sheet/towel/wrap...best to locate the wrap in the trochanteric zone so you can access the posterior ilium. Unfortunately, the C-clamp insertion areas deserve open wound management similar to your open perineal traumatic wound.
An experienced general surgeon is you and your patient's best friend.
Avoid problems whenever you can. Early aggressive yet appropriate intervention facilitates his care.
Two Friday nights ago, we had a nice male Harley rider (for 10 days) wishbone himself with a very similar injury (except some ramus fractures, and larger wound)...we wrapped and packed him, angio'd him, fixed him, washed him thru Pfann, washed him again in the lithotomy position, and then diverted him...we couldn't repair the sphincter...all from 1-4am...always at night...then we just wash him some more from below...it's been a good routine for our patients.
Our general surgeons are tops, and fun to work with.
Open management of the traumatic dependant wound should lower the chance of implant infection.
Keep it simple-
Chip
M.L. Chip Routt, Jr.,M.D.
Professor-Orthopedic Surgery
Harborview Medical Center
Seattle, WA 98104-2499