
Date: Fri, 19 Nov 2004 14:13:25 -0600
From: Steven Rabin
Subject: Distal Humerus Nonunion
Hello all,
This is an 80 year old gentleman without major other medical problems who initially presented to me one year ago with a failed attempt at fixation of comminuted T-type supracondylar humerus fracture. The original surgeon used a single plate and a triceps splitting approach and the surgery failed less than 1 week postop. I don't have those x-rays.
I revised the failed fixation in Nov. 2003. Please see attached file (first revision). The triceps was mangled with its central portion very deficient. I used an olecranon osteotomy.
|
|
My fixation failed in January 2004. Please see attached files (first revision fail).
 |
 |
 |
At surgery it appeared infected. Cultures eventually grew out strep viridans subcultured through broth. It was very hyperemic. I treated it with hardware removal, a spanning plate that was meant to provide temporary stability, and irrigation & debridement x 2. (I did not use an external fixator because of the osteoporosis, and the inability to get stability of the fragments.) An antibiotic impregnated cement spacer was added. Files( after I&D.) Last I&D was in March 2004.
 |
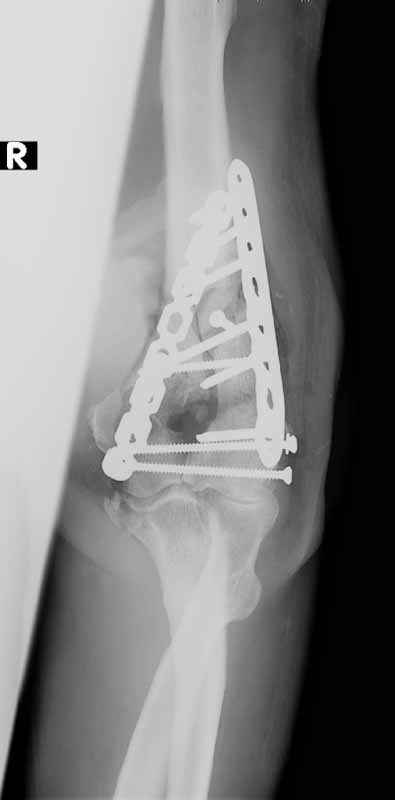
He was treated with IV antibiotics and no sign of infection was seen. After antibiotics were stopped, he still showed no sign of infection. He was offered a total elbow replacement which he refused since he has a handicapped child that he needs to care for, and he did not want to accept the lifting restrictions. He was offered an elbow fusion which he refused because he did not want the stiffness, but he did agree to fixation across the elbow without taking out the joint, even knowing that he would still have stiffness and even with later soft tissue release might not be any different than a fusion. The second revision including cross elbow fixation is in files (2nd revision).
 |
 |
He continues without sign of infection. But his sed rate is 65 and C-reactive protein 21. Despite cast immobilization, his current x-rays (11/17/04) show another failure of fixation (files current)... He still does not want replacement.
 |
 |
Any ideas would be appreciated.
steve rabin
co-chief ortho trauma, Loyola
Date: Fri, 19 Nov 2004 23:01:24 +0000
From: AOBONEDOC
Hello:
Do nothing if possible.
If this is not acceptable, I & D and bisopy offabx, remove all hardware, resect all suspect bone, implantation of abx impregnated absorbable calcium sulfate beads and see how he functions with a resection type arthroplasty. I had one of these work reasonably well once. If resection arthoplasty not functional, fuse (if not infected), consider using BMP. Just some thought off the top of my head.
Sincerely and respectively,
M. Bryan Neal, MD
Arlington Orthopedics and Hand Surgery Specialists, Ltd.
Arlington Heights, Illinois 60005
Date: Sat, 20 Nov 2004 11:49:54 +0500
From: Alexander Chelnokov
Dear Colleague,
ACN> Do nothing if possible.
Why include into reply all images from the original posting?!!!!! And make it twice! Everyone who tried to download 10 Mb via PDA + cell phone would understand me...
Best regards,
Alexander N. Chelnokov
Ural Scientific Research Institute of Traumatology and Orthopaedics
7, Bankovsky str. Ekaterinburg 620014 Russia
Date: Sat, 20 Nov 2004 11:08:44 -0000
From: Nuno Craveiro Lopes
I suggest to use a Ilizarov frame as on this supracondylar pseudarthrosis after a infected plating.
Best regards,
Date: Sat, 20 Nov 2004 11:59:58 -0800
From: Doug Hanel-
Not an easy case.
My suggestions: Better bone carpentry, augmented implant (use a femoral condyle allograft for the anterior block) longer plate with screw spread and an ex fx from deltoid insertion to wrist for 12 weeks.
I'd really like to know the final outcome.
DPH
Douglas Hanel MD
Professor
Hand and Microvascular Surgery
Director Orthopaedic Education
Department of Orthopaedics and Sports Medicine
University of Washington
Date: Sun, 21 Nov 2004 00:23:02 EST
From: Tadabq
In this 80 year old with recalcitrant nonunion distal humerus, broken plate spanning the elbow, and history of infection I suggest:
1. Do nothing until he begins to drain (likely) or accepts resection arthroplasty or arthrodesis.
2. If and when it begins to drain then remove the implant, culture and antibiotics.
3. If and when he subsequently accepts resection arthroplasty or arthrodesis perform it staged with a) repeat debridement (remove infected bone, perhaps the whole distal humerus) b)implant antibiotic spacer c) several more weeks antibiotics d)if no active infection remove spacer and leave with resection arthroplasty or shorten and arthrodese.
TD
Date: Sat, 20 Nov 2004 23:51:14 -0800
From: George Thomas
The only similar case I did landed in a similar position - persistent non-union, though, fortunately, not infected. I would also have said do nothing, except after a look at the case posted by Dr. Nuno, it seems Ilizarov would be a good idea.
All the best,
George Thomas,
Chennai, India
Date: Sat, 20 Nov 2004 22:50:05 +0000
From: Mehmet Arazi
Dear Dr. Rabin:
I would have treated this patient with a hybrid ex-fix. Three or four tensioned small K-wires for distal fragment and 6mm. scahnz screws for proximal humeral shaft fixation. Be careful about radial nerve during placement of schanz screws. Small wires with a crossed placement offers a good fixation even in a osteoporotic bone. The nonunion side also can be grafted with autogenous bone graft. The fixation also can be extended to the proximal forearm. It will work.
Best wishes,
Mehmet Arazi MD,
Selcuk University Medical Faculty,
Dep Orthop & Trauma,
Konya, 42080, TURKIYE
Date: Mon, 22 Nov 2004 13:11:30 -0500
From: James Carr
I agree with the rec to observe for now, and treat specific symptoms as they arise. He could still be infected. Is he diabetic? At this point, he basically has an elbow resection, and I believe that's about all he can ultimately get out of it. As a technical point, I think there is no substitute for right angle medial-lateral plates in the distal humerus. We had a recent case in a diabetic using a company with the precontoured medial-lateral column plates, and he failed in the saggital plane (apex posterior angulation). He promptly healed at revision by using the right angle construct with non prebent plates.
Jim Carr
James B. Carr, MD
Premier Orthopedic Specialists
Columbia, SC 29203
Date: Mon, 22 Nov 2004 12:23:31 -0600
From: Steven Rabin
thanks to all who have answered so far. No diabetes.